

Durable responses and reversible toxicity of high-dose interleukin-2 treatment of melanoma and renal cancer in a Community Hospital Biotherapy Program
- PMID: 24855563
- PMCID: PMC4030280
- DOI: 10.1186/2051-1426-2-13
Durable responses and reversible toxicity of high-dose interleukin-2 treatment of melanoma and renal cancer in a Community Hospital Biotherapy Program
Abstract
Background: High-dose interleukin-2 (IL-2) has been FDA-approved for over 20 years, but it is offered only at a small number of centers with expertise in its administration. We analyzed the outcomes of patients receiving high-dose IL-2 in relation to the severity of toxicity to ascertain if response or survival were adversely affected.
Methods: A retrospective analysis of the outcomes of 500 patients with metastatic renal cell carcinoma (RCC) (n = 186) or melanoma (n = 314) treated with high-dose IL-2 between 1997 and 2012 at Providence Cancer Center was performed. IL-2 was administered at a dose of 600,000 international units per kg by IV bolus every 8 hours for up to 14 doses. A second cycle was administered 16 days after the first and patients with tumor regression could receive additional cycles. Survival and anti-tumor response were analyzed by diagnosis, severity of toxicity, number of IL-2 cycles and subsequent therapy.
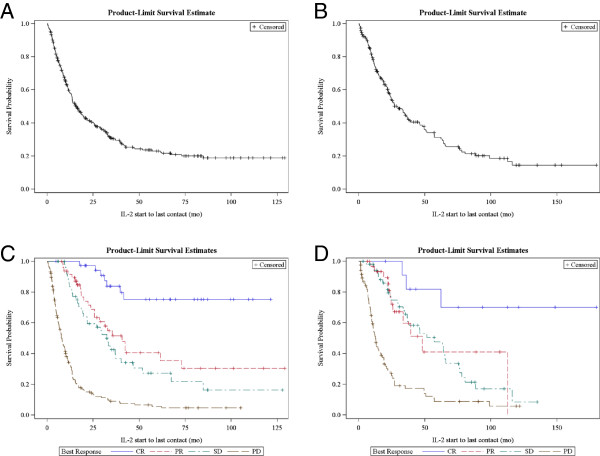
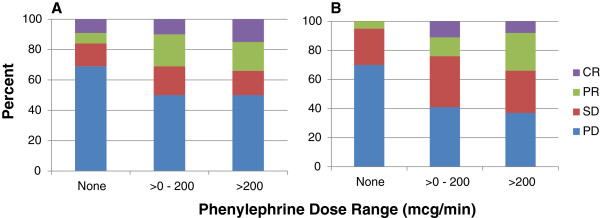
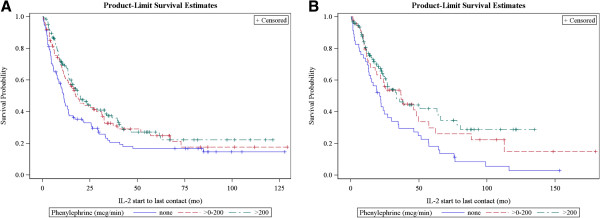
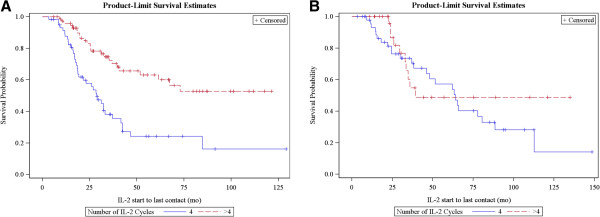
Results: The objective response rate in melanoma was 28% (complete 12% and partial 16%), and in RCC was 24% (complete 7% and partial 17%). The 1-, 2- and 3-year survivals were 59%, 41% and 31%, for melanoma and 75%, 56% and 44%, for RCC, respectively. The proportion of patients with complete or partial response in both melanoma and RCC was higher in patients who a) required higher phenylephrine doses to treat hypotension (p < 0.003), b) developed acidosis (bicarbonate < 19 mmol (p < 0.01)), or c) thrombocytopenia (<50, 50-100, >100,000 platelets; p < 0.025). The proportion achieving a complete or partial response was greater in patients with melanoma who received 5 or more compared with 4 or fewer IL-2 cycles (p < 0.0001). The incidence of death from IL-2 was less than 1% and was not higher in patients who required phenylephrine.
Conclusions: High-dose IL-2 can be administered safely; severe toxicity including hypotension is reversible and can be managed in a community hospital. The tumor response and survival reported here are superior to the published literature and support treating patients to their individualized maximum tolerated dose. IL-2 should remain part of the treatment paradigm in selected patients with melanoma and RCC.
Keywords: Interleukin-2; Melanoma; Renal cancer.
Figures
References
-
- Hodi FS, O’Day SJ, McDermott DF, Weber J, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbé C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–723. doi: 10.1056/NEJMoa1003466. - DOI - PMC - PubMed
-
- Robert C, Thomas L, Bondarenko I, O’Day S, Weber J, Garbe C, Lebbe C, Baurain JF, Testori A, Grob JJ, Davidson N, Richards J, Maio M, Hauschild A, Miller WH Jr, Gascon P, Lotem M, Harmankaya K, Ibrahim R, Francis S, Chen TT, Humphrey R, Hoos A, Wolchok JD. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364:2517–2526. doi: 10.1056/NEJMoa1104621. - DOI - PubMed
-
- Schadendorf D, Hodi FS, Roberts C, Weber JS, Margolin K, Hamid O, Chen TT, Berman DM, Wolchok JD. Pooled analysis of long-term survival data from phase II and phase III trials of ipilimumab in metastatic or locally advanced, unresectable melanoma. European Cancer Congress. 2013. p. LBA24. - PMC - PubMed
-
- Wolchok JD, Kluger H, Callahan MK, Postow MA, Rizvi NA, Lesokhin AM, Segal NH, Ariyan CE, Gordon RA, Reed K, Burke MM, Caldwell A, Kronenberg SA, Agunwamba BU, Zhang X, Lowy I, Inzunza HD, Feely W, Horak CE, Hong Q, Korman AJ, Wigginton JM, Gupta A, Sznol M. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013;369:122–133. doi: 10.1056/NEJMoa1302369. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources