

Reduced risk of hypoglycemia with once-daily glargine versus twice-daily NPH and number needed to harm with NPH to demonstrate the risk of one additional hypoglycemic event in type 2 diabetes: Evidence from a long-term controlled trial
- PMID: 24856612
- PMCID: PMC4802045
- DOI: 10.1016/j.jdiacomp.2014.04.003
Reduced risk of hypoglycemia with once-daily glargine versus twice-daily NPH and number needed to harm with NPH to demonstrate the risk of one additional hypoglycemic event in type 2 diabetes: Evidence from a long-term controlled trial
Abstract
Aims: This analysis evaluated HbA1c-adjusted hypoglycemia risk with glargine versus neutral protamine Hagedorn (NPH) over a 5-year study in patients with Type 2 diabetes mellitus (T2DM). Clinical significance was assessed using number needed to harm (NNH) to demonstrate the risk of one additional patient experiencing at least one hypoglycemic event.
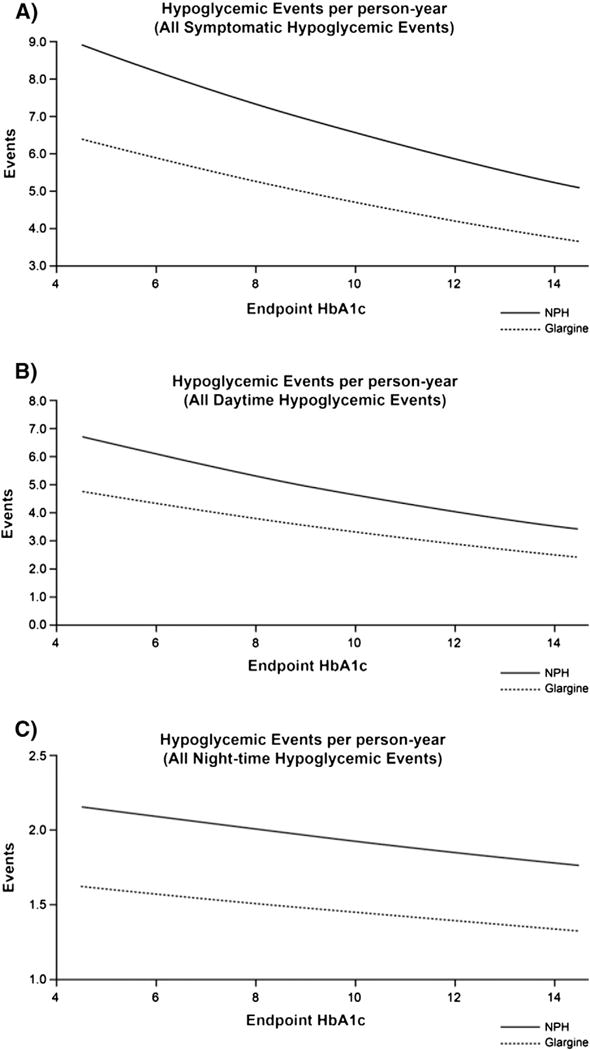
Methods: Individual patient-level data for symptomatic documented hypoglycemia and HbA1c values from a 5-year randomized study comparing once-daily glargine (n=513) with twice-daily NPH (n=504) were analyzed. Symptomatic hypoglycemia was categorized according to concurrent self-monitoring blood glucose levels and need for assistance. Hypoglycemic events per patient-year as a function of HbA1c were fitted by negative binomial regression using treatment and HbA1c at endpoint as independent variables. An estimate of NNH was derived from logistic regression models.
Results: The cumulative number of symptomatic hypoglycemia events was consistently lower with glargine compared with NPH over 5years. Compared with twice-daily NPH, once-daily glargine treatment resulted in significantly lower adjusted odds ratios (OR) for all daytime hypoglycemia (OR 0.74; p=0.030) and any severe event (OR 0.64; p=0.035), representing a 26% and 36% reduction in the odds of daytime and severe hypoglycemia, respectively. Our model predicts that, if 25 patients were treated with NPH instead of glargine, then one additional patient would experience at least one severe hypoglycemic event.
Conclusions: This analysis of long-term insulin treatment confirms findings from short-term studies and demonstrates that glargine provides sustained, clinically meaningful reductions in risk of hypoglycemia compared with NPH in patients with T2DM.
Keywords: Clinical diabetes; Clinical science and care; Glargine; Hypoglycemia; NPH.
Copyright © 2014 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: J Rosenstock has served on scientific advisory boards and received honorarium or consulting fees from Roche, Sanofi, Novo Nordisk, Eli Lilly and Company, MannKind, GlaxoSmithKline, Takeda, Daiichi Sankyo, Johnson & Johnson, Novartis and Boehringer Ingelheim, and Amylin Pharmaceuticals. He has also received grants/research support from Merck, Pfizer, Sanofi, Novo Nordisk, Roche, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Takeda, Novartis, AstraZeneca, Amylin Pharmaceuticals, Johnson & Johnson, Daiichi Sankyo, MannKind, Intarcia Therapeutics and Boehringer Ingelheim. V Fonseca has received research support (to Tulane University) with grants from Novo Nordisk, Sanofi, Eli Lilly and Company, Daiichi Sankyo, Pamlabs, Reata Pharmaceuticals and Halozyme, and honoraria for consulting and lectures from GlaxoSmithKline, Takeda, Sanofi, Novo Nordisk, Daiichi Sankyo, Pamlabs, Xoma, AstraZeneca and Eli Lilly and Company. S Schinzel and MP Dain are employees of Sanofi. P Mullins has received grants and/or honoraria for consulting from Astra Zeneca, Boehringer Ingelheim, Merck, Novartis, Roche and Sanofi. M Riddle has received grants for research and/or honoraria for consulting or lectures from Amylin Pharmaceuticals, Eli Lilly and Company, the Amylin Lilly Alliance, Novo Nordisk, Pfizer, Sanofi and Valeritas; this conflict of interest has been reviewed and managed by Oregon Health & Science University.
Figures


References
-
- Ali M, White J, Lee CH, Palmer JL, Smith-Palmer J, Fakhoury W, et al. Therapy conversion to biphasic insulin aspart 30 improves long-term outcomes and reduces the costs of type 2 diabetes in Saudi Arabia. Journal of Medical Economics. 2008;11:651–670. - PubMed
-
- Allicar MP, Megas F, Houzard S, Baroux A, Le Thai F, Augendre-Ferrante B. Frequency and costs of hospital stays for hypoglycemia in France in 1995. Presse Médicale. 2000;29:657–661. - PubMed
-
- Bazzano LA, Lee LJ, Shi L, Reynolds K, Jackson JA, Fonseca V. Safety and efficacy of glargine compared with NPH insulin for the treatment of type 2 diabetes: A meta-analysis of randomized controlled trials. Diabetic Medicine. 2008;25:924–932. - PubMed
-
- Bullano MF, Al-Zakwani IS, Fisher MD, Menditto L, Willey VJ. Differences in hypoglycemia event rates and associated cost-consequence in patients initiated on long-acting and intermediate-acting insulin products. Current Medical Research and Opinion. 2005;21:291–298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
