

Impact of non-cardiovascular disease comorbidity on cardiovascular disease symptom severity: a population-based study
- PMID: 24856803
- PMCID: PMC4078220
- DOI: 10.1016/j.ijcard.2014.05.001
Impact of non-cardiovascular disease comorbidity on cardiovascular disease symptom severity: a population-based study
Abstract
Objectives: Non-cardiovascular comorbidity is common in cardiovascular disease (CVD) populations but its influence on chest pain (CP) and shortness of breath (SOB) symptom-specific physical limitations is unknown. We wanted to test the a priori hypothesis that an unrelated comorbidity would influence symptom-specific physical limitations and to investigate this impact in different severities of CVD.
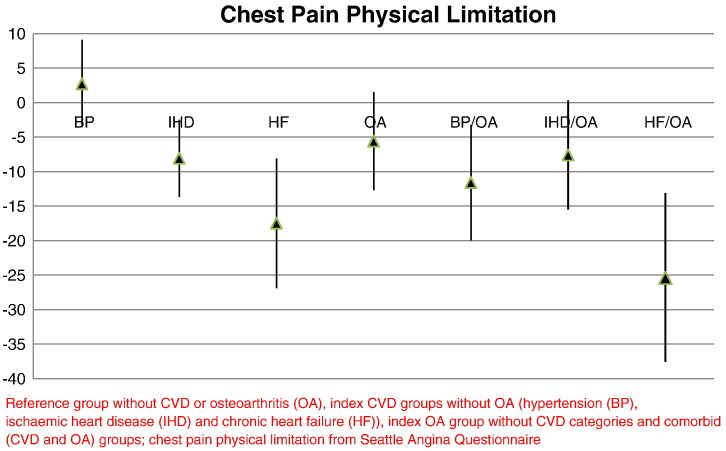
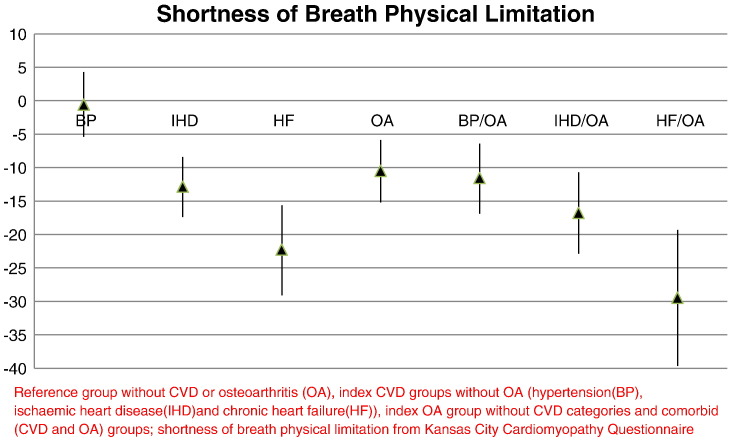
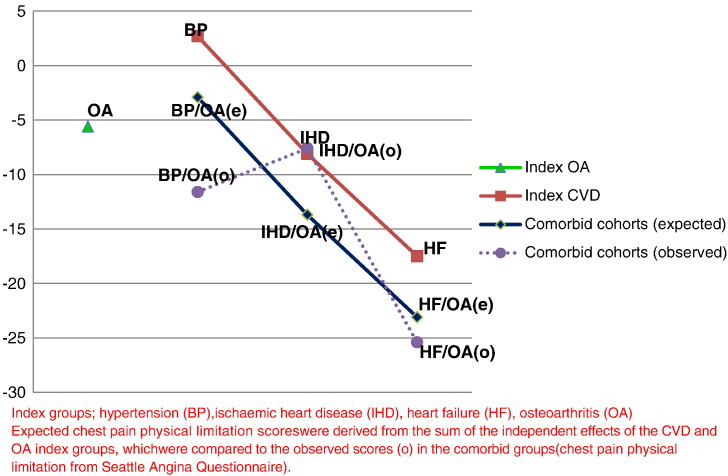
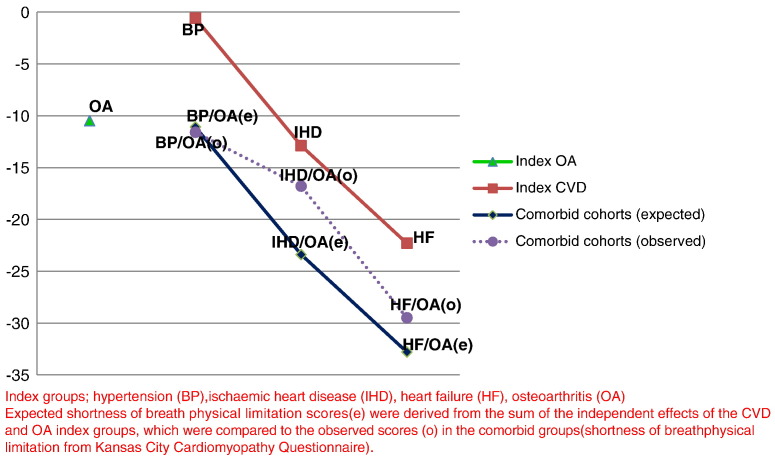
Method and results: The study was based on 5426 patients from ten family practices, organised into eight a priori exclusive severity groups: (i) no CVD or osteoarthritis (OA) (reference), (ii) index hypertension, ischaemic heart disease (IHD) and heart failure (HF) without OA, (iii) index OA without CVD and (iv) same CVD groups with comorbid OA. The measure of CP physical limitations was Seattle Angina Questionnaire and for SOB physical limitations was the Kansas City Cardiomyopathy Questionnaire. Adjusted baseline associations between the cohorts and symptom-specific physical limitations were assessed using linear regression methods. In the study population, 1443 (27%) reported CP and 2097 (39%) SOB. CP and SOB physical limitations increased with CVD severity in the index and comorbid groups. Compared with the respective index CVD group, the CP physical limitation scores for comorbid CVD groups with OA were lower by: -14.7 (95% CI -21.5, 7.8) for hypertension, -5.5 (-10.4, -0.7) for IHD and -22.1 (-31.0, -6.7) for HF. For SOB physical limitations, comorbid scores were lower by: -9.2 (-13.8, -4.6) for hypertension, -6.4 (-11.1, -1.8) for IHD and -8.8 (-19.3, 1.65) for HF.
Conclusions: CP and SOB are common symptoms, and OA increases the CVD symptom-specific physical limitations additively. Comorbidity interventions need to be developed for CVD specific health outcomes.
Keywords: Cardiovascular diseases; Comorbidity; Health status; Osteoarthritis.
Copyright © 2014. Published by Elsevier Ireland Ltd.
Figures
References
-
- Ong K., Wu B., Cheung B., Barter P., Rye K. Arthritis: its prevalence, risk factors, and association with cardiovascular diseases in the United States, 1999 to 2008. Ann Epidemiol. 2013;23(2):80–86. - PubMed
-
- Alonso J., Ferrer M., Gandek B. Health-related quality of life associated with chronic conditions in eight countries: results from the International Quality of Life Assessment (IQOLA) Project. Qual Life Res. 2004;13(2):283–298. - PubMed
-
- Kadam U., Croft P. Clinical comorbidity in osteoarthritis: associations with physical function in older patients in family practice. J Rheumatol. 2007;34(9):1899–1904. - PubMed
-
- Jonsson H., Helgadottir G.P., Aspelund T. Hand osteoarthritis in older women is associated with carotid and coronary atherosclerosis: the AGES Reykjavik Study. Ann Rheum Dis. 2009;68(11):1696–1700. - PubMed
-
- Kadam U.T., Holmberg A., Blagojevic M., Nilsson P.M., Akesson K. Risk factors for cardiovascular disease and future osteoarthritis-related arthroplasty: a population-based cohort study in men and women from Malmo, Sweden. Scand J Rheumatol. 2011;40(6):478–485. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
