

Patient-derived xenograft models in gynecologic malignancies
- PMID: 24857111
- PMCID: PMC4156101
- DOI: 10.14694/EdBook_AM.2014.34.e258
Patient-derived xenograft models in gynecologic malignancies
Abstract
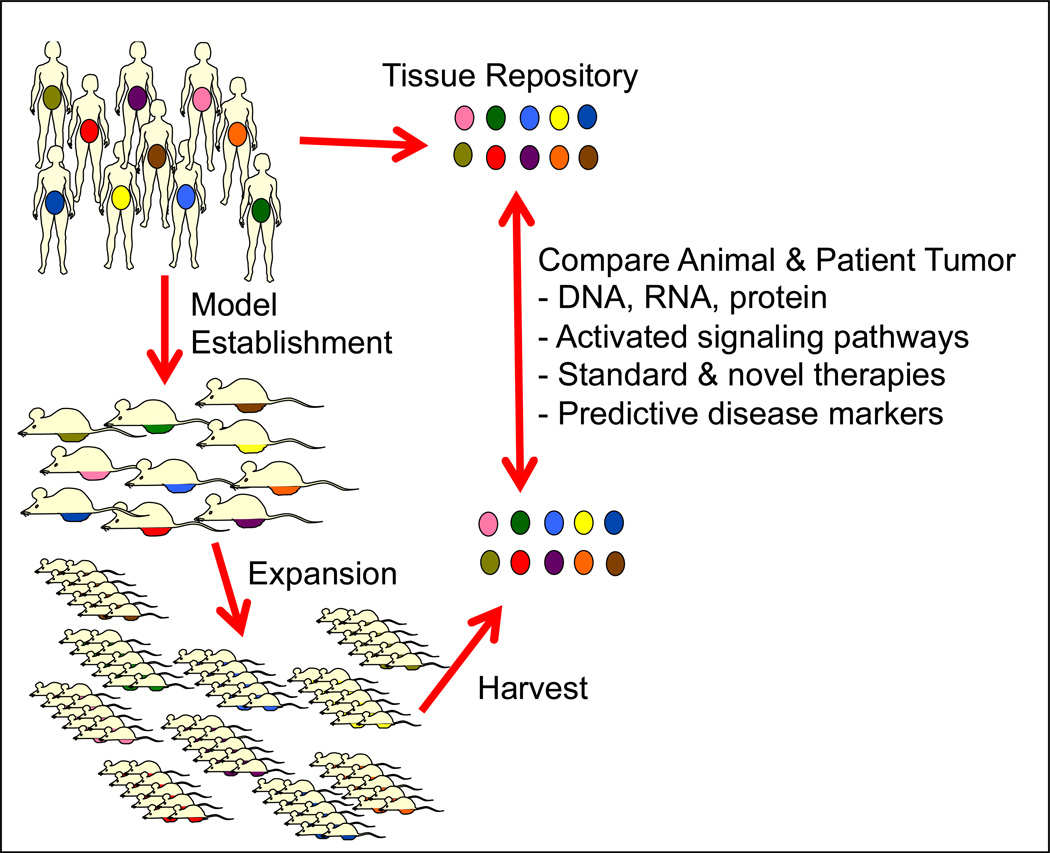
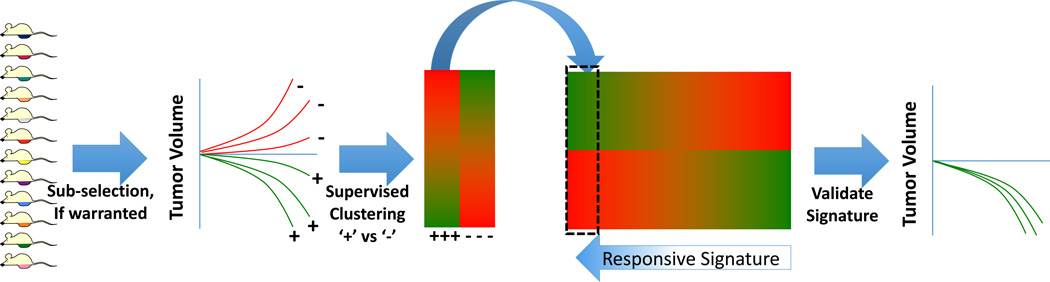
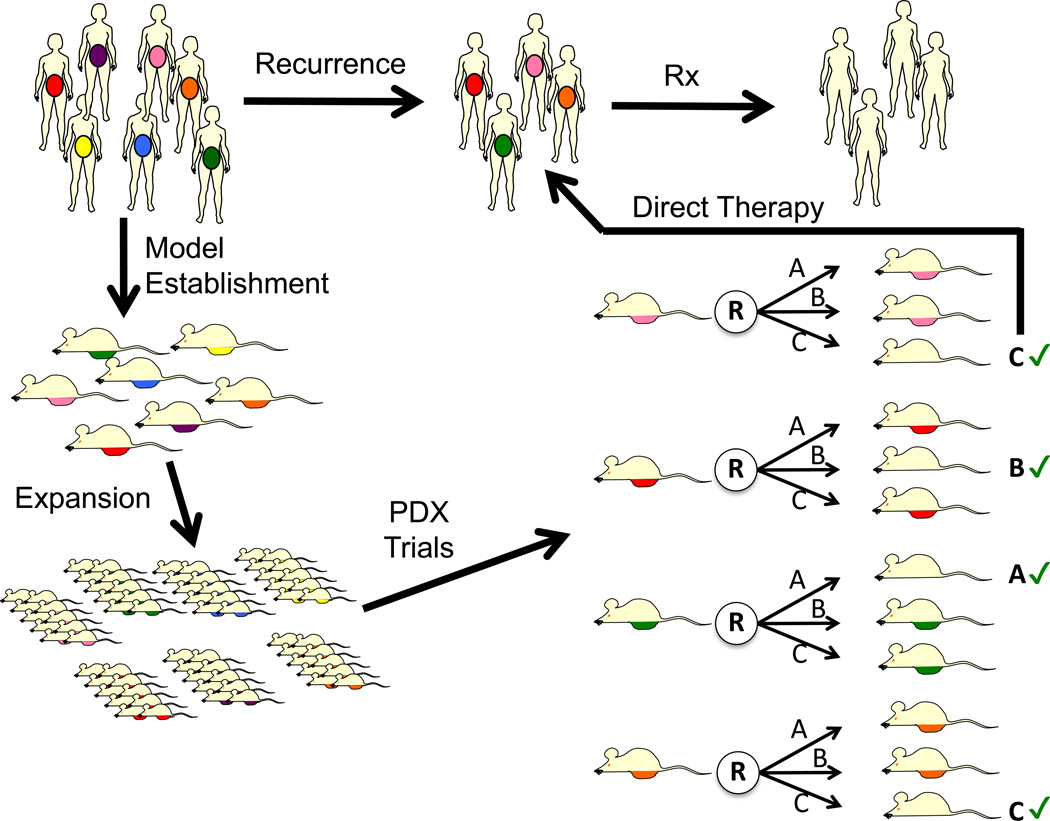
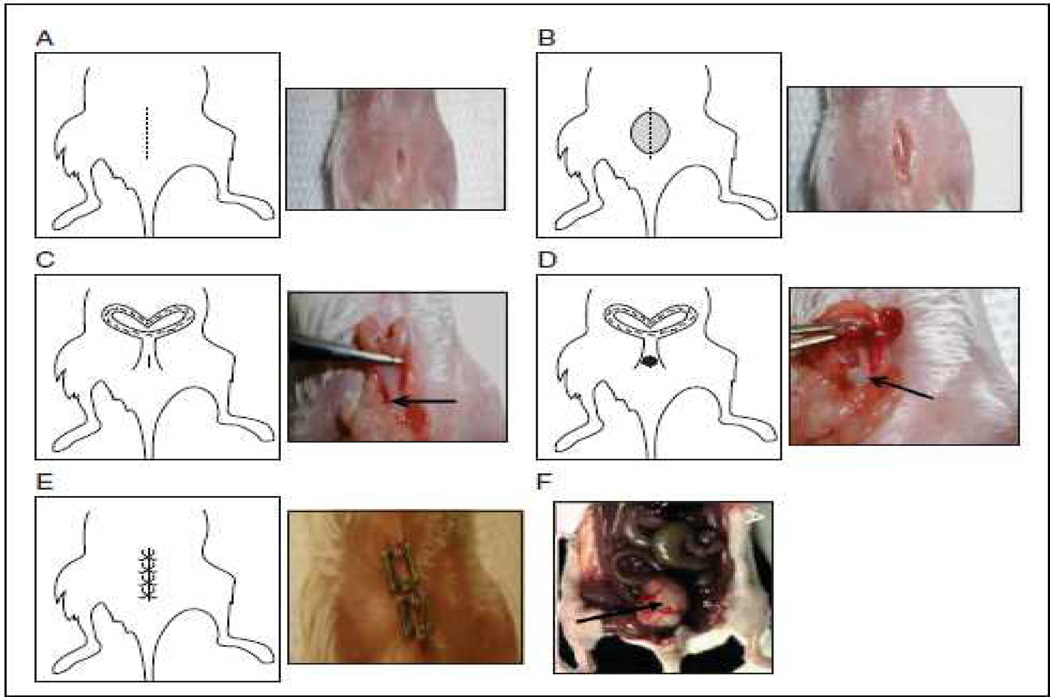
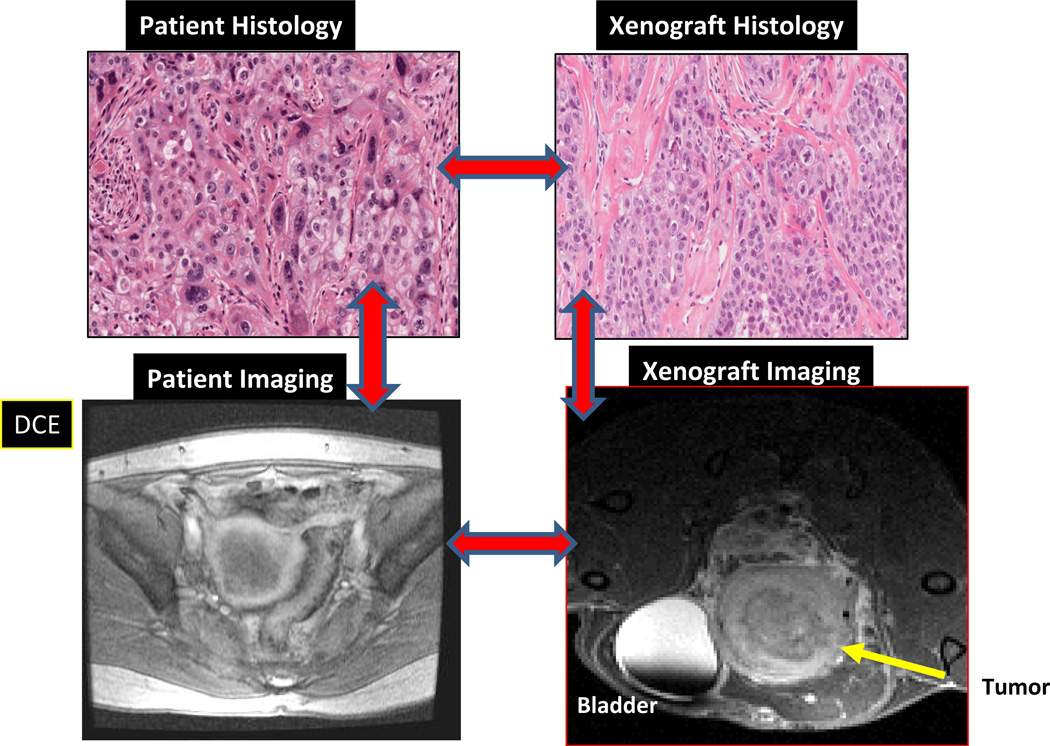
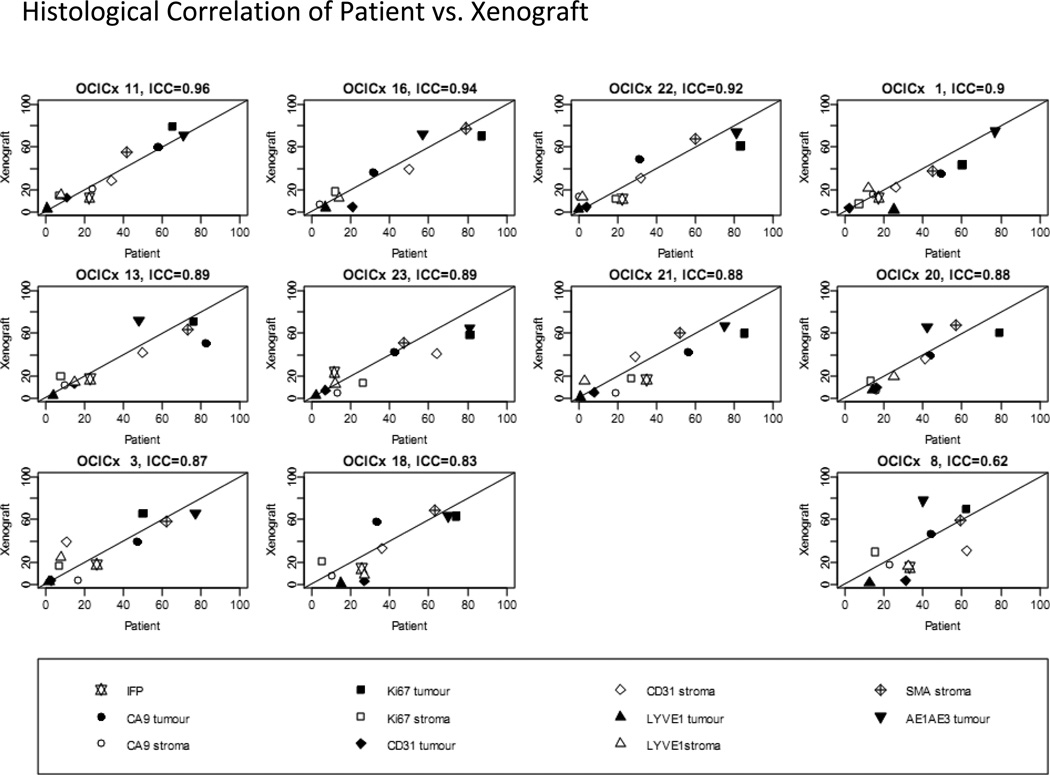
In the era of targeted therapies, patients with gynecologic malignancies have not yet been major beneficiaries of this new class of agents. This may reflect the fact that the main tumor types-ovarian, uterine, and cervical--are a highly heterogeneous group of cancers with variable response to standard chemotherapies and the lack of models in which to study the diversity of these cancers. Cancer-derived cell lines fail to adequately recapitulate molecular hallmarks of specific cancer subsets and complex microenvironments, which may be critical for sensitivity to targeted therapies. Patient-derived xenografts (PDX) generated from fresh human tumor without prior in vitro culture, combined with whole genome expression, gene copy number, and sequencing analyses, could dramatically aid the development of novel therapies for gynecologic malignancies. Gynecologic tumors can be engrafted in immunodeficient mice with a high rate of success and within a reasonable time frame. The resulting PDX accurately recapitulates the patient's tumor with respect to histologic, molecular, and in vivo treatment response characteristics. Orthotopic PDX develop complications relevant to the clinic, such as ascites and bowel obstruction, providing opportunities to understand the biology of these clinical problems. Thus, PDX have great promise for improved understanding of gynecologic malignancies, serve as better models for designing novel therapies and clinical trials, and could underpin individualized, directed therapy for patients from whom such models have been established.
Conflict of interest statement
CLS receives in-kind collaborative laboratory support from Clovis Oncology.
PH is an unpaid consultant for Tesaro and Clovis Oncology and receives research funding from Tesaro, Clovis Oncology and Genentech.
Figures
References
-
- Adams RA. Heightened Immunity and Susceptibility toward Cheek Pouch Heterografts of a Mouse Leukemia in Syrian Hamsters. Cancer Res. 1963;23:1834–1840. - PubMed
-
- Carrel S, Sordat B, Merenda C. Establishment of a cell line (Co-115) from a human colon carcinoma transplanted into nude mice. Cancer Res. 1976;36:3978–3984. - PubMed
-
- Weroha SJ, Becker MA, Enderica-Gonzalez S, Harrington SC, Oberg AL, Maurer MJ, Perkins S, Al Hilli M, Butler K, McKinstry S, Fink SR, Jenkins RB, Hou X, Kalli KR, Goodman KM, Sarkaria JN, Karlan BY, Kumar A, Kaufmann SH, Hartmann LC, Haluska P. Tumorgrafts as in vivo surrogates for women with ovarian cancer. Clin Cancer Res. 2014 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
