

Combination of morphologic criteria and α-fetoprotein in selection of patients with hepatocellular carcinoma for liver transplantation minimizes the problem of posttransplant tumor recurrence
- PMID: 24858191
- PMCID: PMC4161934
- DOI: 10.1007/s00268-014-2647-3
Combination of morphologic criteria and α-fetoprotein in selection of patients with hepatocellular carcinoma for liver transplantation minimizes the problem of posttransplant tumor recurrence
Abstract
Background: Serum α-fetoprotein concentration (AFP) might be a useful addition to morphologic criteria for selecting patients with hepatocellular carcinoma (HCC) for liver transplantation (LT). The aim of this study was to evaluate the role of AFP in selecting HCC patients at minimal risk of posttransplant tumor recurrence in the setting of existing criteria.
Methods: This retrospective cohort study was based on 121 HCC patients after LT performed at a single institution. AFP was evaluated as a predictor of posttransplant tumor recurrence with respect to fulfillment of the Milan, University of California, San Francisco (UCSF), and Up-to-7 criteria.
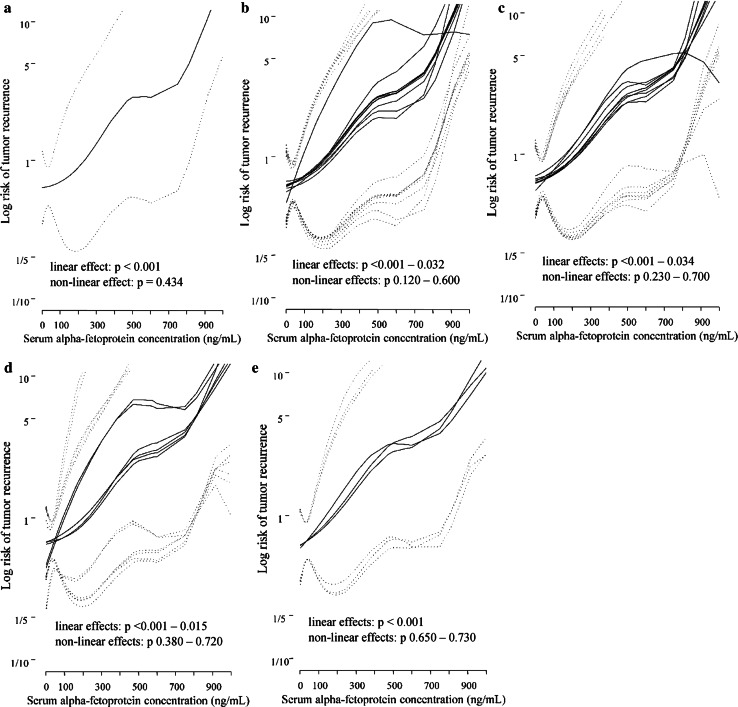
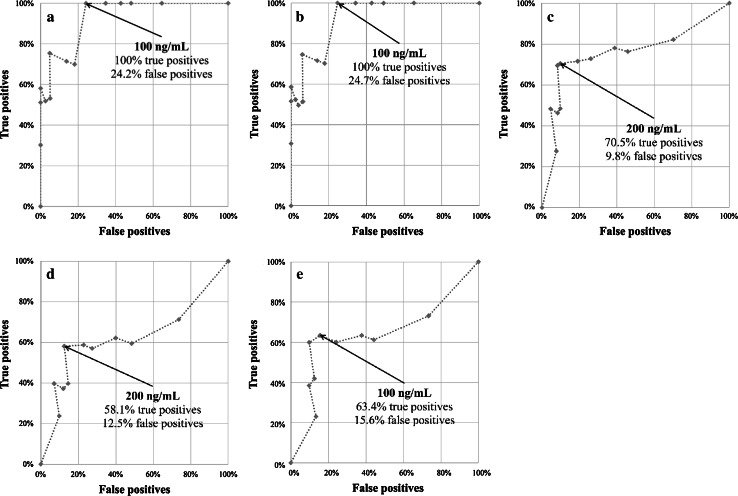
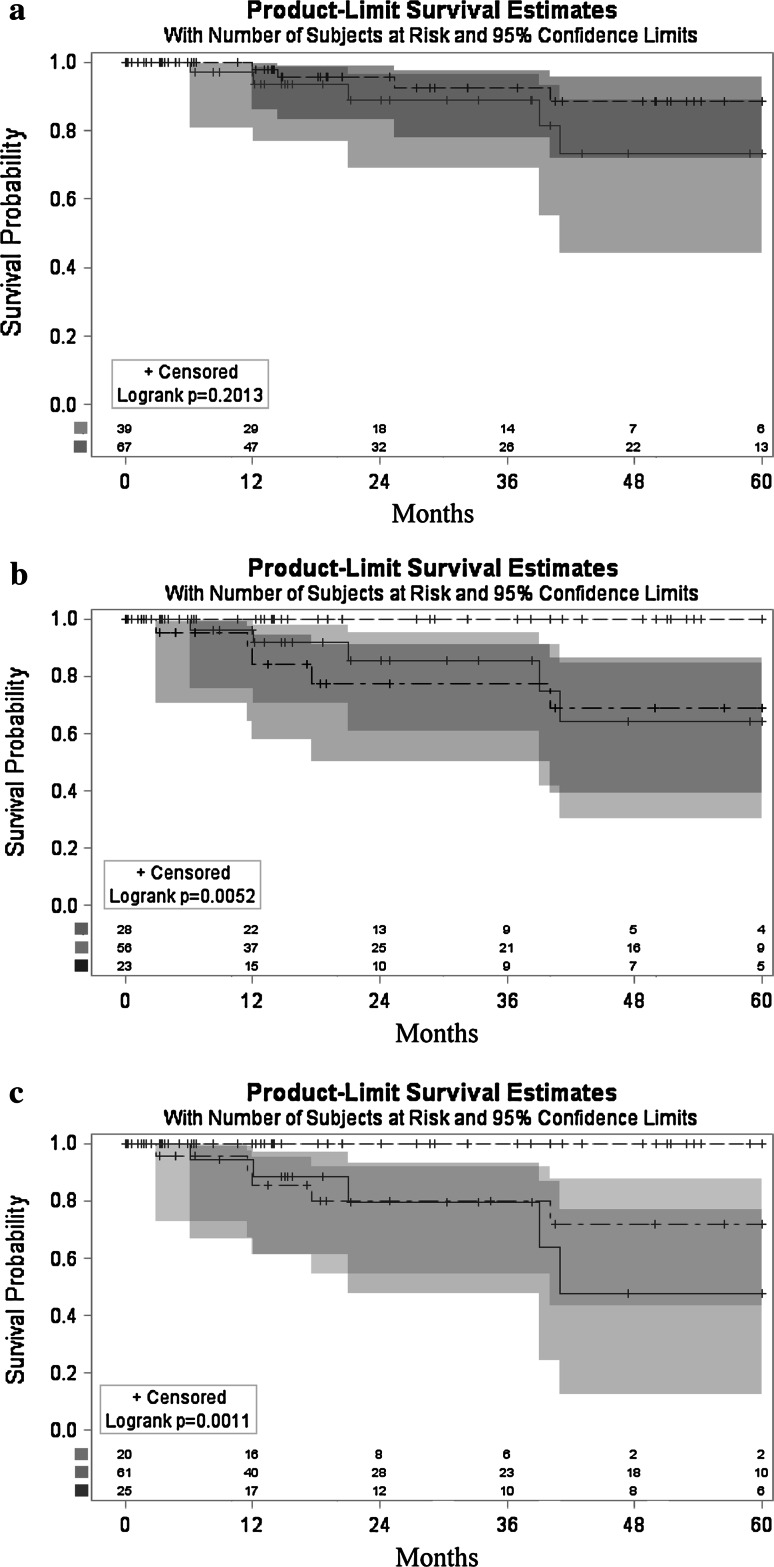
Results: There was a nearly linear association between AFP and the risk of HCC recurrence (p < 0.001 for linear effect; p = 0.434 for nonlinear effect). AFP predicted HCC recurrence in patients (1) beyond the Milan criteria (p < 0.001; optimal cutoff 200 ng/ml); (2) within the UCSF criteria (p = 0.001; optimal cutoff 100 ng/ml) and beyond them (p = 0.015; optimal cutoff 200 ng/ml); and (3) within the Up-to-7 criteria (p = 0.001; optimal cutoff 100 ng/ml) and beyond them (p = 0.023; optimal cutoff 100 ng/ml) but not in patients within the Milan criteria (p = 0.834). Patients within either UCSF and Up-to-7 criteria with AFP level <100 ng/ml exhibited superior (100 %) 5-year recurrence-free survival-significantly higher than those within UCSF (p = 0.005) or Up-to-7 (p = 0.001) criteria with AFP levels higher than the estimated cutoffs or beyond with AFP levels less than the estimated cutoffs.
Conclusions: Combining the UCSF and Up-to-7 criteria with an AFP level <100 ng/ml is associated with minimal risk of tumor recurrence. Hence, this combination might be useful for selecting HCC patients for LT.
Figures
Similar articles
-
Alpha-fetoprotein level > 1000 ng/mL as an exclusion criterion for liver transplantation in patients with hepatocellular carcinoma meeting the Milan criteria.Liver Transpl. 2014 Aug;20(8):945-51. doi: 10.1002/lt.23904. Epub 2014 Jul 12. Liver Transpl. 2014. PMID: 24797281 Free PMC article.
-
Evaluation of Patients With Hepatocellular Carcinomas That Do Not Produce α-Fetoprotein.JAMA Surg. 2017 Jan 1;152(1):55-64. doi: 10.1001/jamasurg.2016.3310. JAMA Surg. 2017. PMID: 27706479
-
Homocysteine: A novel prognostic biomarker in liver transplantation for alpha-fetoprotein- negative hepatocellular carcinoma.Cancer Biomark. 2020;29(2):197-206. doi: 10.3233/CBM-201545. Cancer Biomark. 2020. PMID: 32623388
-
Patient Selection for Downstaging of Hepatocellular Carcinoma Prior to Liver Transplantation-Adjusting the Odds?Transpl Int. 2022 Apr 21;35:10333. doi: 10.3389/ti.2022.10333. eCollection 2022. Transpl Int. 2022. PMID: 35529597 Free PMC article. Review.
-
Do We Need to Be Limited by Matching Milan Criteria for Survival in Living Donor Liver Transplantation?J Gastrointest Cancer. 2020 Dec;51(4):1107-1113. doi: 10.1007/s12029-020-00482-0. J Gastrointest Cancer. 2020. PMID: 32857265 Review.
Cited by
-
Hepatocellular carcinoma beyond Milan criteria: Management and transplant selection criteria.World J Hepatol. 2016 Jul 28;8(21):874-80. doi: 10.4254/wjh.v8.i21.874. World J Hepatol. 2016. PMID: 27478537 Free PMC article.
-
The Landscape Of Alpha Fetoprotein In Hepatocellular Carcinoma: Where Are We?Int J Biol Sci. 2022 Jan 1;18(2):536-551. doi: 10.7150/ijbs.64537. eCollection 2022. Int J Biol Sci. 2022. PMID: 35002508 Free PMC article. Review.
-
Contribution of alpha-fetoprotein in liver transplantation for hepatocellular carcinoma.World J Hepatol. 2016 Jul 28;8(21):881-90. doi: 10.4254/wjh.v8.i21.881. World J Hepatol. 2016. PMID: 27478538 Free PMC article. Review.
-
Obtaining Optimal Long-Term Outcomes from Liver Transplantation for Hepatocellular Cancer.Dig Dis Sci. 2019 Apr;64(4):976-984. doi: 10.1007/s10620-019-05550-5. Dig Dis Sci. 2019. PMID: 30840163 Review.
-
Hepatocellular carcinoma - time to take the ticket.World J Gastrointest Surg. 2019 Jun 27;11(6):287-295. doi: 10.4240/wjgs.v11.i6.287. World J Gastrointest Surg. 2019. PMID: 31367276 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
