

Postartesunate delayed hemolysis is a predictable event related to the lifesaving effect of artemisinins
- PMID: 24859359
- PMCID: PMC4093678
- DOI: 10.1182/blood-2014-02-555953
Postartesunate delayed hemolysis is a predictable event related to the lifesaving effect of artemisinins
Abstract
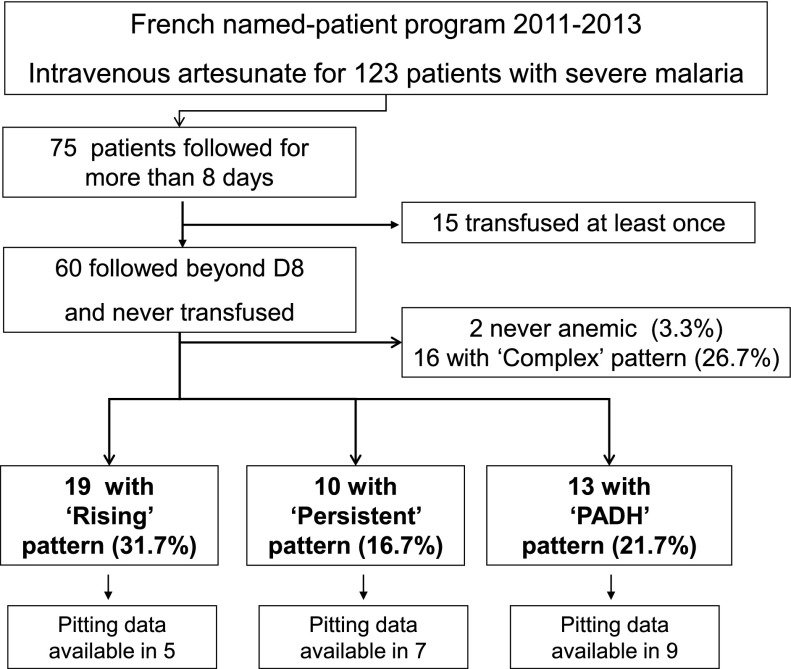
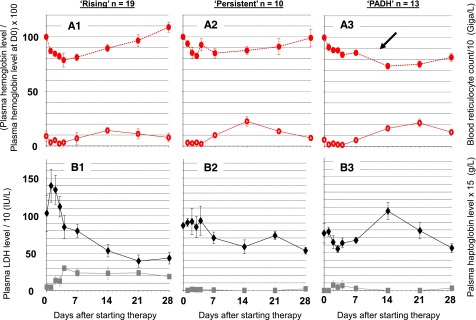
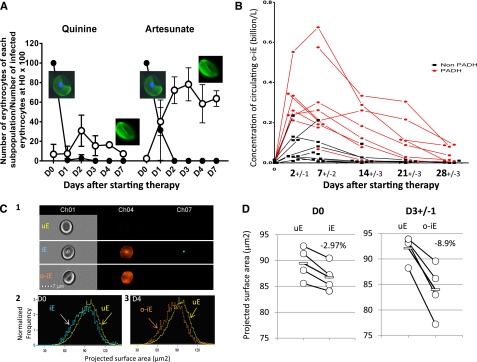
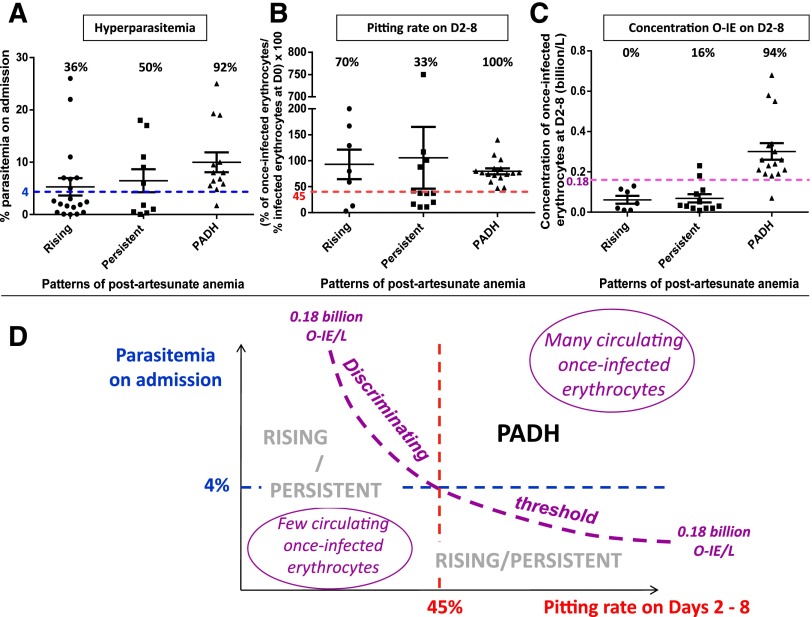
Patients with severe malaria treated with artesunate sometimes experience a delayed hemolytic episode. Artesunate (AS) induces pitting, a splenic process whereby dead parasites are expelled from their host erythrocytes. These once-infected erythrocytes then return to the circulation. We analyzed hematologic parameters in 123 travelers treated with AS for severe malaria. Among 60 nontransfused patients observed for more than 8 days, 13 (22%) had delayed hemolysis. The peak concentration of circulating once-infected erythrocytes was measured during the first week in 21 patients and was significantly higher in 9 patients with delayed hemolysis than in 12 with other patterns of anemia (0.30 vs 0.07; P = .0001). The threshold of 180 million once-infected erythrocytes per liter discriminated patients with delayed hemolysis with 89% sensitivity and 83% specificity. Once-infected erythrocyte morphology analyzed by using ImageStream in 4 patients showed an 8.9% reduction in their projected area, an alteration likely contributing to their shorter lifespan. Delayed clearance of infected erythrocytes spared by pitting during AS treatment is an original mechanism of hemolytic anemia. Our findings consolidate a disease framework for posttreatment anemia in malaria in which delayed hemolysis is a new entity. The early concentration of once-infected erythrocytes is a solid candidate marker to predict post-AS delayed hemolysis.
© 2014 by The American Society of Hematology.
Figures
Comment in
-
Case definition: postartemisinin delayed hemolysis.Blood. 2014 Jul 10;124(2):157-8. doi: 10.1182/blood-2014-06-578922. Blood. 2014. PMID: 25013158 Free PMC article.
References
-
- WHO. The treatment of malaria. 2nd ed. Geneva, Switzerland: WHO Press; 2010.
-
- Dondorp A, Nosten F, Stepniewska K, Day N, White N South East Asian Quinine Artesunate Malaria Trial (SEAQUAMAT) group. Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial. Lancet. 2005;366(9487):717–725. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
