

The Theranostic Path to Personalized Nanomedicine
- PMID: 24860796
- PMCID: PMC4031631
- DOI: 10.1007/s40336-014-0051-5
The Theranostic Path to Personalized Nanomedicine
Abstract
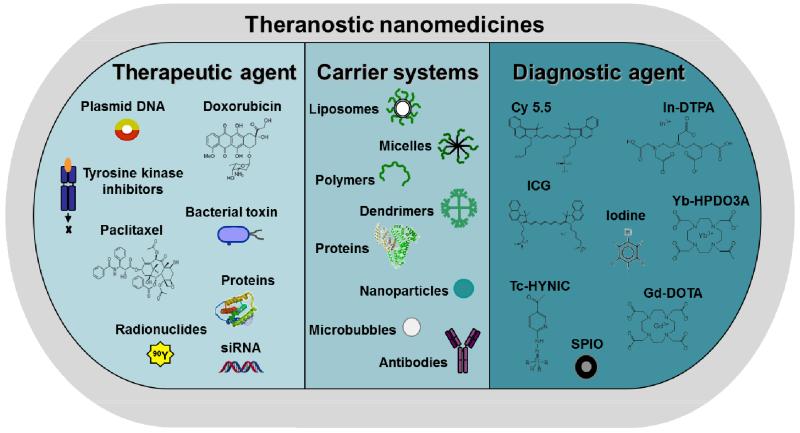
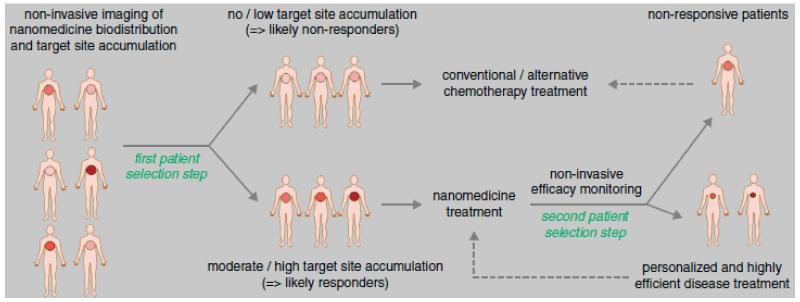
Advances in nanotechnology and chemical engineering have led to the development of many different drug delivery systems. These 1-100(0) nm-sized carrier materials aim to increase drug concentrations at the pathological site, while avoiding their accumulation in healthy non-target tissues, thereby improving the balance between the efficacy and the toxicity of systemic (chemo-) therapeutic interventions. An important advantage of such nanocarrier materials is the ease of incorporating both diagnostic and therapeutic entities within a single formulation, enabling them to be used for theranostic purposes. We here describe the basic principles of using nanomaterials for targeting therapeutic and diagnostic agents to pathological sites, and we discuss how nanotheranostics and image-guided drug delivery can be used to personalize nanomedicine treatments.
Keywords: Drug targeting; Image-guided drug delivery; Nanomedicine; Personalized medicine; Theranostics.
Figures
References
-
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. - PubMed
-
- Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100(1):57–70. - PubMed
-
- Essenberg JM. Cigarette smoke and the incidence of primary neoplasm of the lung in the albino mouse. Science. 1952;116(3021):561–562. - PubMed
-
- Fearon ER. Molecular genetics of colorectal cancer. Annu Rev Pathol. 2011;6:479–507. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources