

Stability of end-of-life preferences: a systematic review of the evidence
- PMID: 24861560
- PMCID: PMC8243894
- DOI: 10.1001/jamainternmed.2014.1183
Stability of end-of-life preferences: a systematic review of the evidence
Abstract
Importance: Policies and practices that promote advance care planning and advance directive completion implicitly assume that patients' choices for end-of-life (EOL) care are stable over time, even with changes in health status.
Objective: To systematically evaluate the evidence on the stability of EOL preferences over time and with changes in health status.
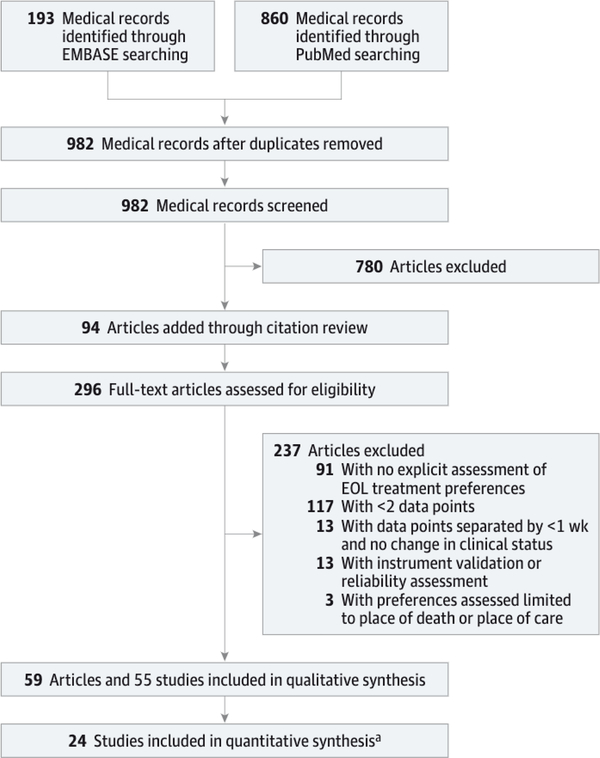
Evidence review: We searched for longitudinal studies of patients' preferences for EOL care in PubMed, EMBASE, and using citation review. Studies restricted to preferences regarding the place of care at the EOL were excluded.
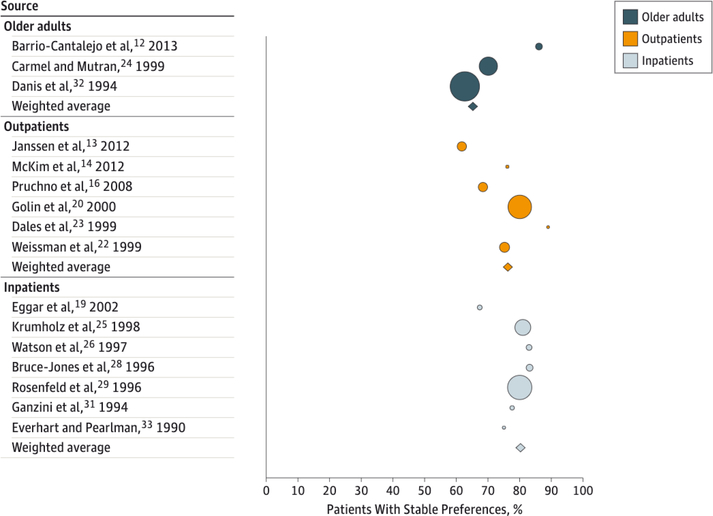
Findings: A total of 296 articles were assessed for eligibility, and 59 met inclusion criteria. Twenty-four articles had sufficient data to extract or calculate the percentage of individuals with stable preferences or the percentage of total preferences that were stable over time. In 17 studies (71%) more than 70% of patients' preferences for EOL care were stable over time. Preference stability was generally greater among inpatients and seriously ill outpatients than among older adults without serious illnesses (P < .002). Patients with higher education and who had engaged in advance care planning had greater preference stability, and preferences to forgo therapies were generally more stable than preferences to receive therapies. Among 9 of the 24 studies (38%) assessing changes in health status, no consistent relationship with preference changes was identified.
Conclusions and relevance: Considerable variability among studies in the methods of preference assessment, the time between assessments, and the definitions of stability preclude meta-analytic estimates of the stability of patients' preferences and the factors influencing these preferences. Although more seriously ill patients and those who engage in advance care planning most commonly have stable preferences for future treatments, further research in real-world settings is needed to confirm the utility of advance care plans for future decision making.
Conflict of interest statement
Figures
Comment in
-
What should be the goal of advance care planning?JAMA Intern Med. 2014 Jul;174(7):1093-4. doi: 10.1001/jamainternmed.2014.1887. JAMA Intern Med. 2014. PMID: 24861458 No abstract available.
References
-
- Ditto PH, Smucker WD, Danks JH, et al. Stability of older adults’ preferences for life-sustaining medical treatment. Health Psychol. 2003;22(6): 605–615. - PubMed
-
- Houts RM. Smucker WD, Jacobson JA. Ditto PH. Danks JH. Predicting elderly outpatients’ life-sustaining treatment preferences over time: the majority rules. Med Decis Making. 2002;22(1):39–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
