

A comparison of live counseling with a web-based lifestyle and medication intervention to reduce coronary heart disease risk: a randomized clinical trial
- PMID: 24861959
- PMCID: PMC4142754
- DOI: 10.1001/jamainternmed.2014.1984
A comparison of live counseling with a web-based lifestyle and medication intervention to reduce coronary heart disease risk: a randomized clinical trial
Abstract
Importance: Most primary care clinicians lack the skills and resources to offer effective lifestyle and medication (L&M) counseling to reduce coronary heart disease (CHD) risk. Thus, effective and feasible CHD prevention programs are needed for typical practice settings.
Objective: To assess the effectiveness, acceptability, and cost-effectiveness of a combined L&M intervention to reduce CHD risk offered in counselor-delivered and web-based formats.
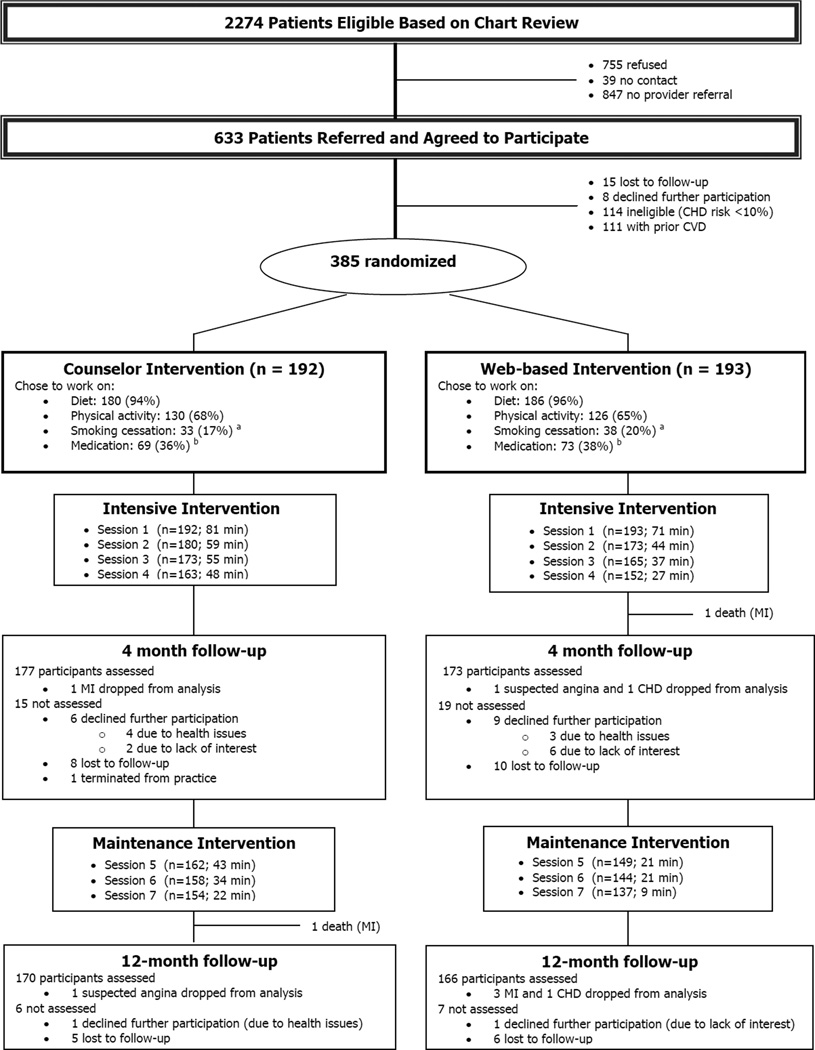
Design, setting, and participants: A comparative effectiveness trial in 5 diverse family medicine practices in North Carolina. Participants were established patients, aged 35 to 79 years, with no known cardiovascular disease, and at moderate to high risk for CHD (10-year Framingham Risk Score [FRS], ≥10%).
Interventions: Participants were randomized to counselor-delivered or web-based format, each including 4 intensive and 3 maintenance sessions. After randomization, both formats used a web-based decision aid showing potential CHD risk reduction associated with L&M risk-reducing strategies. Participants chose the risk-reducing strategies they wished to follow.
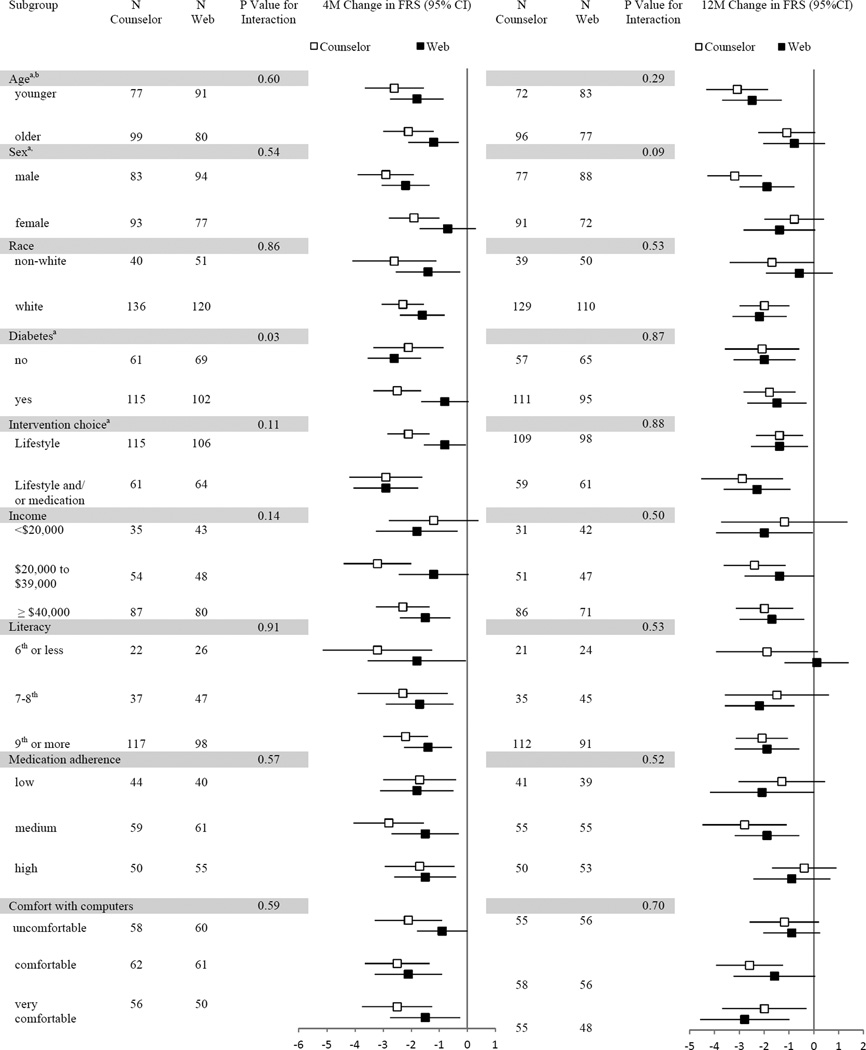
Main outcomes and measures: The primary outcome was within-group change in FRS at 4-month follow-up. Other measures included standardized assessments of blood pressure, blood lipid levels, lifestyle behaviors, and medication adherence. Acceptability and cost-effectiveness were also assessed. Outcomes were assessed at 4 and 12 months.
Results: Of 2274 screened patients, 385 were randomized (192 counselor; 193 web): mean age, 62 years; 24% African American; and mean FRS, 16.9%. Follow-up at 4 and 12 months included 91% and 87% of the randomized participants, respectively. There was a sustained reduction in FRS at both 4 months (primary outcome) and 12 months for both counselor-based (-2.3% [95% CI, -3.0% to -1.6%] and -1.9% [95% CI, -2.8% to -1.1%], respectively) and web-based groups (-1.5% [95% CI, -2.2% to -0.9%] and -1.7% [95% CI, -2.6% to -0.8%] respectively). At 4 months, the adjusted difference in FRS between groups was -1.0% (95% CI, -1.8% to -0.1%) (P = .03), and at 12 months, it was -0.6% (95% CI, -1.7% to 0.5%) (P = .30). The 12-month costs from the payer perspective were $207 and $110 per person for the counselor- and web-based interventions, respectively.
Conclusions and relevance: Both intervention formats reduced CHD risk through 12-month follow-up. The web format was less expensive.
Trial registration: clinicaltrials.gov Identifier: NCT01245686.
Conflict of interest statement
Conflict of interest: none
Figures
Comment in
-
Live vs electronically delivered weight-loss interventions: paying for feasible interventions.JAMA Intern Med. 2014 Jul;174(7):1157-9. doi: 10.1001/jamainternmed.2014.414. JAMA Intern Med. 2014. PMID: 24861172 Free PMC article. No abstract available.
References
-
- Estruch R, Ros E, Salas-Salvado J, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013;368(14):1279–1290. - PubMed
-
- Gueyffier F, Froment A, Gouton M. New meta-analysis of treatment trials of hypertension: improving the estimate of therapeutic benefit. J Hum Hypertens. 1996;10(1):1–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
