

Uncontrolled asthma and recurring pulmonary opacities: just asthma?
- PMID: 24862414
- PMCID: PMC4039853
- DOI: 10.1136/bcr-2013-202428
Uncontrolled asthma and recurring pulmonary opacities: just asthma?
Abstract
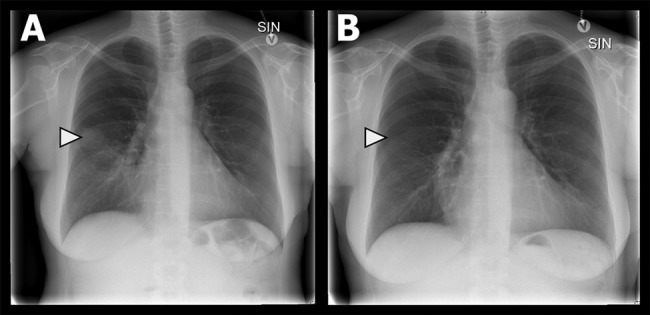
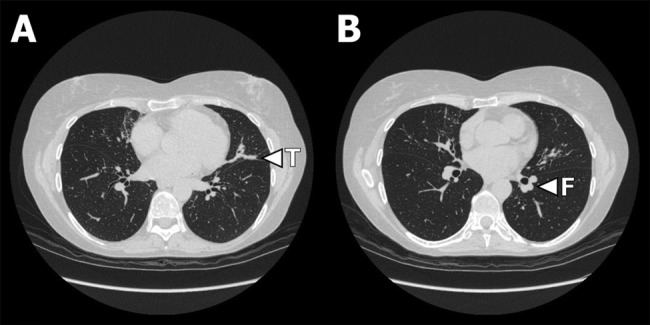
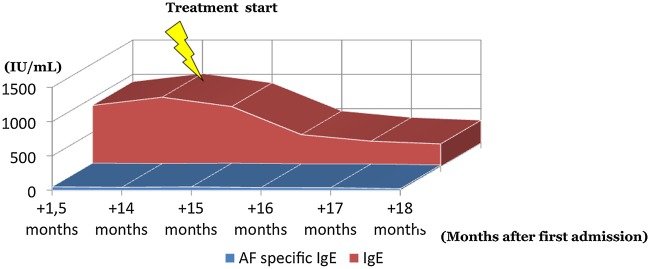
In asthma, when comorbidities and common causes of poor control have been considered and treated, the clinician may speculate, 'Is it all asthma?'. In patients with uncontrolled atopic asthma with recurring episodes of symptoms mimicking pneumonia, the suspicion of allergic bronchopulmonary aspergillosis (ABPA) should remain high. ABPA is caused by a complex immunological hypersensitivity reaction to colonisation with Aspergillus fumigatus in the bronchial tree, and is characterised by the presence of atopic asthma, blood eosinophilia, migrating pulmonary opacities and potential bronchiectasis. This case report describes a delay in diagnosing ABPA which was imitating pneumonia. The clinician should pay increased attention to ABPA and test for this in patients with uncontrolled asthma with an ongoing requirement for oral corticosteroids and/or antibiotics and with pulmonary opacities on chest imaging.
2014 BMJ Publishing Group Ltd.
Figures
References
-
- Bel EH. Clinical phenotypes of asthma. Curr Opin Pulm Med 2004;10:44–50 - PubMed
-
- Cazzoletti L, Marcon A, Janson C, et al. Asthma control in Europe: a real-world evaluation based on an international population-based study. J Allergy Clin Immunol 2007;120:1360–7 - PubMed
-
- Agarwal R. Allergic bronchopulmonary aspergillosis. Chest 2009;135:805–26 - PubMed
-
- Rosenberg M, Patterson R, Mintzer R, et al. Clinical and immunologic criteria for the diagnosis of allergic bronchopulmonary aspergillosis. Ann Intern Med 1977;86:405–14 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical