

Anti-inflammatory therapies for cardiovascular disease
- PMID: 24864079
- PMCID: PMC4155455
- DOI: 10.1093/eurheartj/ehu203
Anti-inflammatory therapies for cardiovascular disease
Abstract
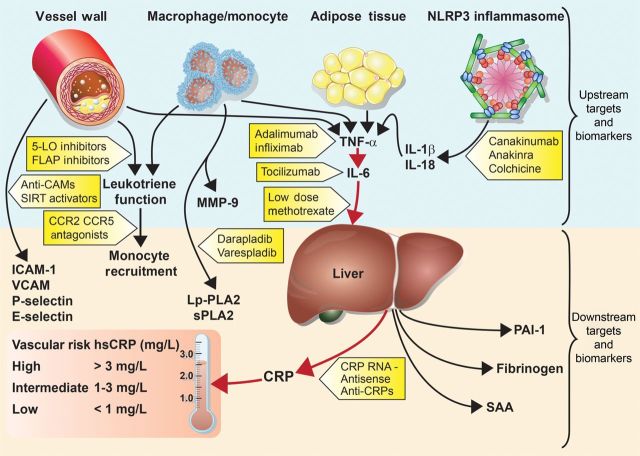
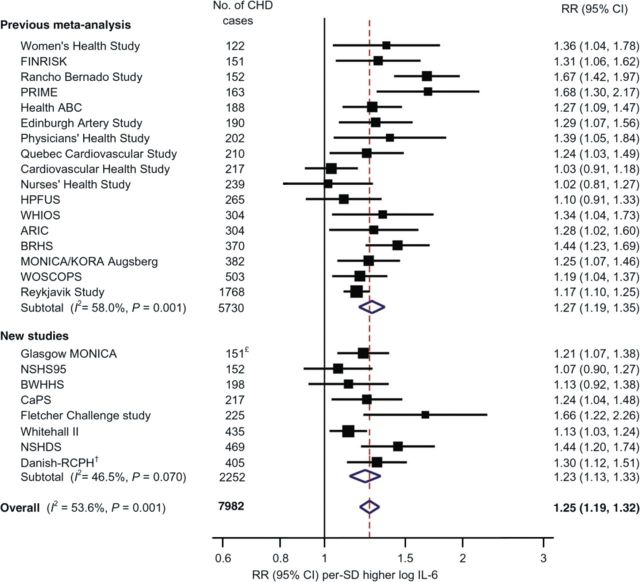
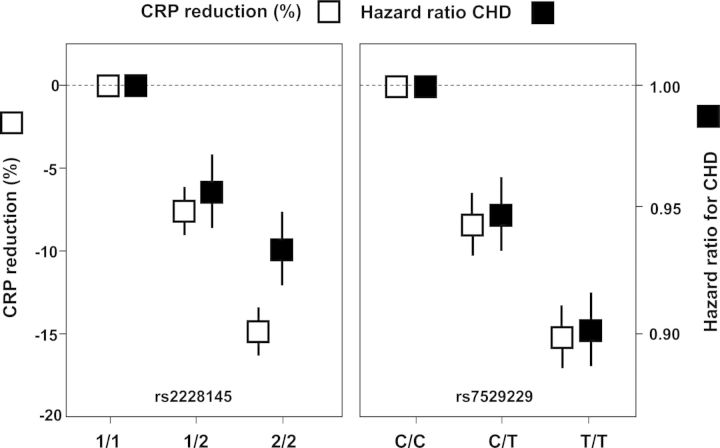
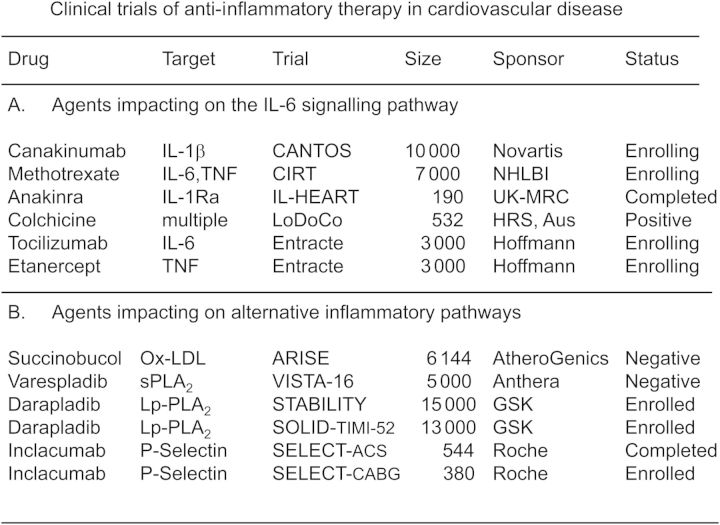
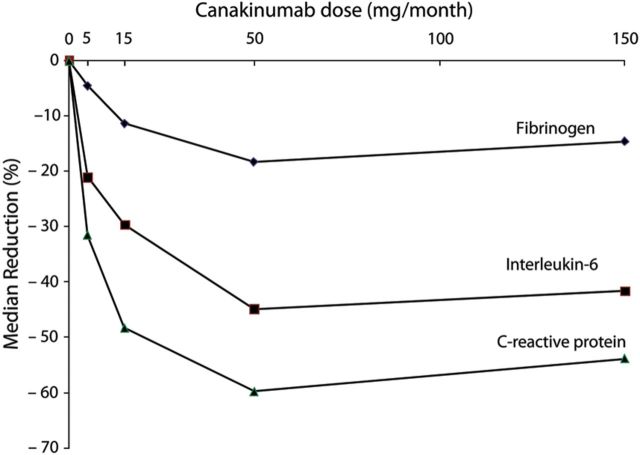
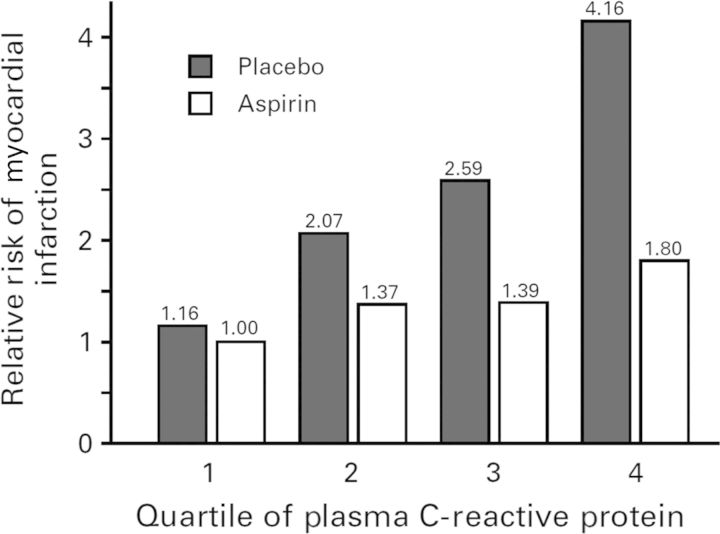
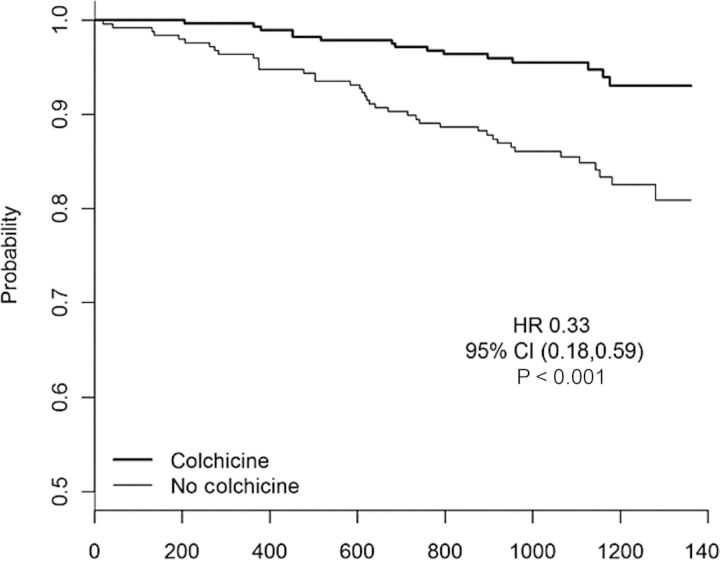
Atherothrombosis is no longer considered solely a disorder of lipoprotein accumulation in the arterial wall. Rather, the initiation and progression of atherosclerotic lesions is currently understood to have major inflammatory influences that encompass components of both the innate and acquired immune systems. Promising clinical data for 'upstream' biomarkers of inflammation such as interleukin-6 (IL-6) as well as 'downstream' biomarkers such as C-reactive protein, observations regarding cholesterol crystals as an activator of the IL-1β generating inflammasome, and recent Mendelian randomization data for the IL-6 receptor support the hypothesis that inflammatory mediators of atherosclerosis may converge on the central IL-1, tumour necrosis factor (TNF-α), IL-6 signalling pathway. On this basis, emerging anti-inflammatory approaches to vascular protection can be categorized into two broad groups, those that target the central IL-6 inflammatory signalling pathway and those that do not. Large-scale Phase III trials are now underway with agents that lead to marked reductions in IL-6 and C-reactive protein (such as canakinumab and methotrexate) as well as with agents that impact on diverse non-IL-6-dependent pathways (such as varespladib and darapladib). Both approaches have the potential to benefit patients and reduce vascular events. However, care should be taken when interpreting these trials as outcomes for agents that target IL-6 signalling are unlikely to be informative for therapies that target alternative pathways, and vice versa. As the inflammatory system is redundant, compensatory, and crucial for survival, evaluation of risks as well as benefits must drive the development of agents in this class.
Keywords: Atherosclerosis; C reactive protein; Canakinumab; Colchicine; Darapladib; Inflammasome; Inflammation; Interleukin-6; Methotrexate; Salsalate.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2014. For permissions please email: Journals.permissions@oup.com.
Figures
References
-
- Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature. 2011;473:317–325. - PubMed
-
- Ghattas A, Griffiths HR, Devitt A, Lip GY, Shantsila E. Monocytes in coronary artery disease and atherosclerosis: where are we now? JACC. 2013;62:1541–1551. - PubMed
-
- Ridker PM, Rifai N, Stampfer MJ, Hennekens CH. Plasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy men. Circulation. 2000;101:1767–1772. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
