

Molecular mechanisms of liver fibrosis in HIV/HCV coinfection
- PMID: 24865485
- PMCID: PMC4100089
- DOI: 10.3390/ijms15069184
Molecular mechanisms of liver fibrosis in HIV/HCV coinfection
Abstract
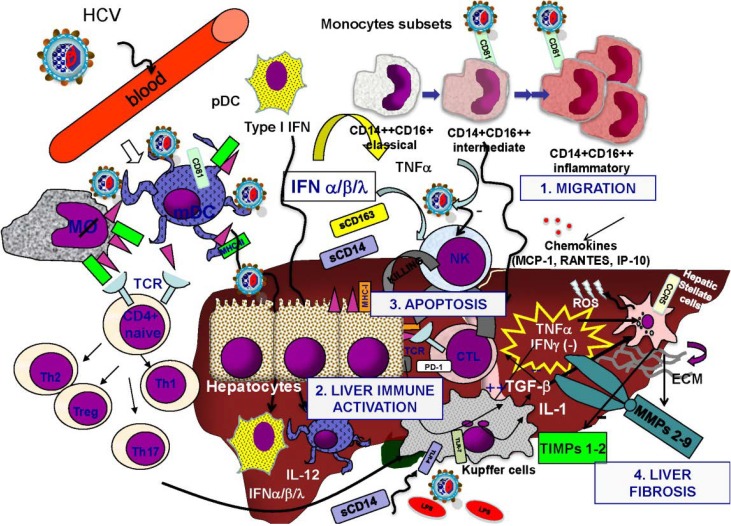
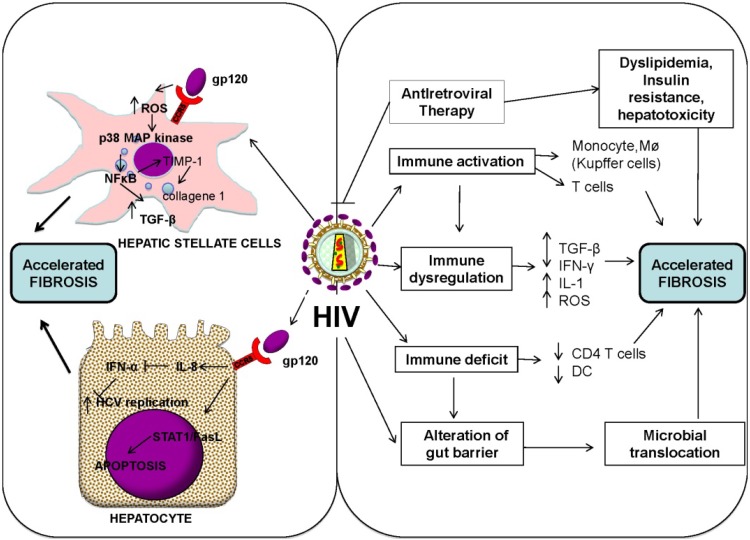
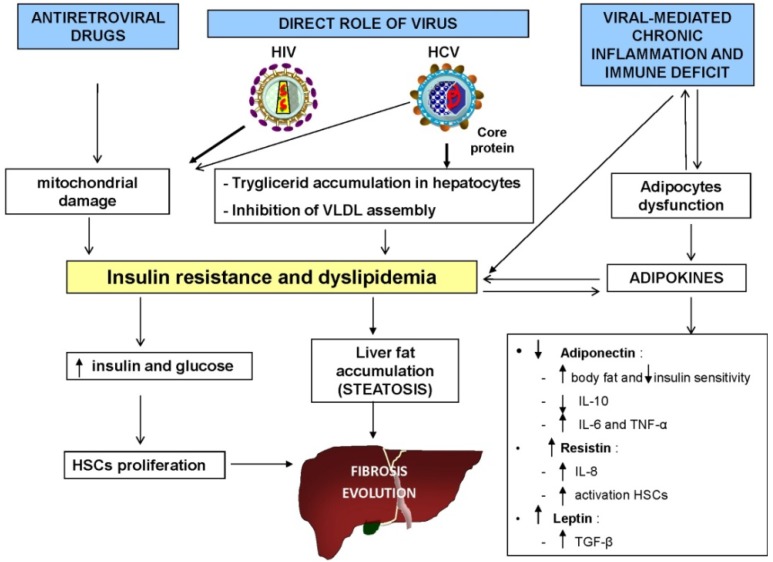
Chronic hepatitis C virus (HCV) infection is an important cause of morbidity and mortality in people coinfected with human immunodeficiency virus (HIV). Several studies have shown that HIV infection promotes accelerated HCV hepatic fibrosis progression, even with HIV replication under full antiretroviral control. The pathogenesis of accelerated hepatic fibrosis among HIV/HCV coinfected individuals is complex and multifactorial. The most relevant mechanisms involved include direct viral effects, immune/cytokine dysregulation, altered levels of matrix metalloproteinases and fibrosis biomarkers, increased oxidative stress and hepatocyte apoptosis, HIV-associated gut depletion of CD4 cells, and microbial translocation. In addition, metabolic alterations, heavy alcohol use, as well drug use, may have a potential role in liver disease progression. Understanding the pathophysiology and regulation of liver fibrosis in HIV/HCV co-infection may lead to the development of therapeutic strategies for the management of all patients with ongoing liver disease. In this review, we therefore discuss the evidence and potential molecular mechanisms involved in the accelerated liver fibrosis seen in patients coinfected with HIV and HCV.
Figures
References
-
- Benhamou Y., Bochet M., di Martino V., Charlotte F., Azria F., Coutellier A., Vidaud M., Bricaire F., Opolon P., Katlama C., et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. Hepatology. 1999;30:1054–1058. doi: 10.1002/hep.510300409. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
