

Is potential malnutrition associated with septic failure and acute infection after revision total joint arthroplasty?
- PMID: 24867449
- PMCID: PMC4390916
- DOI: 10.1007/s11999-014-3685-8
Is potential malnutrition associated with septic failure and acute infection after revision total joint arthroplasty?
Abstract
Background: Although malnutrition has been hypothesized to increase the risk of periprosthetic joint infection (PJI), strong evidence linking the two is lacking.
Questions/purposes: The purposes of this study were to determine (1) if one or more laboratory values suggestive of malnutrition is independently associated with being revised for an infected joint arthroplasty as opposed to for an aseptic failure; (2) the relationship between laboratory parameters suggestive of malnutrition and obesity; and (3) if one or more laboratory parameters suggestive of malnutrition is independently associated with acute PJI complicating an aseptic revision procedure.
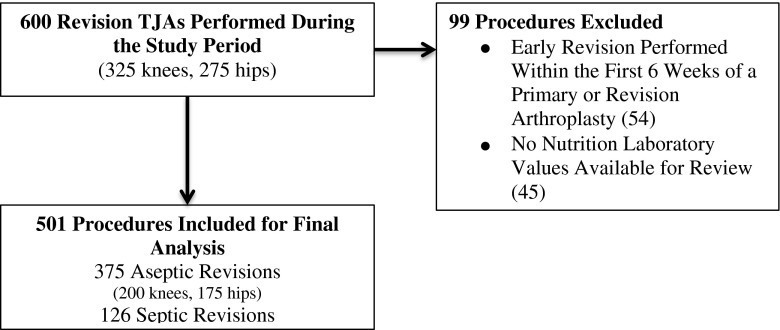
Methods: Between 2002 and 2010, one surgeon performed 600 revision total joint arthroplasties in 547 patients; during that time, nutritional parameters (including serum albumin, total lymphocyte count, and transferrin) were routinely obtained preoperatively; complete data sets were available on 454 patients (501 procedures [84%]). We compared the frequency of having one or more laboratory parameters suggestive of malnutrition between patients undergoing a revision for septic reasons and aseptic reasons as well as between obese and nonobese patients. The 375 aseptic revisions were then assessed for the incidence of acute postoperative infection (within 90 days, diagnosed with Musculoskeletal Infection Society criteria). Multivariate logistic regression modeling was used to evaluate factors independently associated with (1) a septic as opposed to an aseptic mode of failure; and (2) acute postoperative infection after an aseptic revision.
Results: Patients in 67 of 126 (53%) revisions for PJI had one or more laboratory parameters suggestive of malnutrition compared with 123 of 375 (33%) undergoing revision for a noninfectious etiology (odds ratio [OR], 2.3 [95% confidence interval, 1.5-3.5]; p<0.001). Patients who were of normal weight at the time of revision had the highest frequency of laboratory parameters suggestive of malnutrition (42 of 82 [51%]), although this was common in obese patients as well (76 of 238 [32%]) (p=0.002). Among the 375 aseptic revisions, 12 developed an acute postoperative infection (3%). The frequency of infection was nine of 123 in the group having one or more laboratory parameters suggestive of malnutrition and three of 252 in the group not having such laboratory parameters (7% versus 1%; p=0.003). Multivariate regression revealed that having laboratory parameters suggestive of malnutrition is independently associated with both chronic PJI (p=0.003; OR, 2.1) and an acute postoperative infection complicating an aseptic revision arthroplasty (p=0.02; OR, 5.9).
Conclusions: Having one or more laboratory parameters suggestive of malnutrition is common among patients undergoing revision arthroplasty and is independently associated with both chronic septic failure and acute postoperative infection complicating a revision performed for a noninfectious etiology. Future studies should assess the impact of a standardized screening protocol with subsequent correction of abnormal laboratory parameters suggestive of malnutrition on the risk of PJI to determine a potential causal relationship between the two.
Level of evidence: Level III, prognostic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures
Comment in
-
CORR Insights®: Is potential malnutrition associated with septic failure and acute infection after revision total joint arthroplasty?Clin Orthop Relat Res. 2015 Jan;473(1):183-4. doi: 10.1007/s11999-014-3752-1. Epub 2014 Jun 28. Clin Orthop Relat Res. 2015. PMID: 24973087 Free PMC article. No abstract available.
Similar articles
-
Prosthesis failure within 2 years of implantation is highly predictive of infection.Clin Orthop Relat Res. 2013 Nov;471(11):3672-8. doi: 10.1007/s11999-013-3200-7. Epub 2013 Aug 1. Clin Orthop Relat Res. 2013. PMID: 23904245 Free PMC article.
-
Is Hypoalbuminemia Associated With Septic Failure and Acute Infection After Revision Total Joint Arthroplasty? A Study of 4517 Patients From the National Surgical Quality Improvement Program.J Arthroplasty. 2016 May;31(5):963-7. doi: 10.1016/j.arth.2015.11.025. Epub 2015 Nov 26. J Arthroplasty. 2016. PMID: 26718779
-
A Novel Biomarker to Screen for Malnutrition: Albumin/Fibrinogen Ratio Predicts Septic Failure and Acute Infection in Patients Who Underwent Revision Total Joint Arthroplasty.J Arthroplasty. 2021 Sep;36(9):3282-3288. doi: 10.1016/j.arth.2021.04.027. Epub 2021 Apr 30. J Arthroplasty. 2021. PMID: 33992479
-
Risk of Infection After Septic and Aseptic Revision Total Knee Arthroplasty: A Systematic Review.J Bone Joint Surg Am. 2023 Oct 18;105(20):1630-1637. doi: 10.2106/JBJS.23.00361. Epub 2023 Aug 24. J Bone Joint Surg Am. 2023. PMID: 37616387
-
Does the Alpha Defensin ELISA Test Perform Better Than the Alpha Defensin Lateral Flow Test for PJI Diagnosis? A Systematic Review and Meta-analysis of Prospective Studies.Clin Orthop Relat Res. 2020 Jun;478(6):1333-1344. doi: 10.1097/CORR.0000000000001225. Clin Orthop Relat Res. 2020. PMID: 32324670 Free PMC article.
Cited by
-
Modifiable and Nonmodifiable Predictive Factors Associated with the Outcomes of Total Knee Arthroplasty.Joints. 2019 Feb 1;7(1):13-18. doi: 10.1055/s-0039-1678563. eCollection 2019 Mar. Joints. 2019. PMID: 31879725 Free PMC article. Review.
-
The significance of the vitamin D metabolism in the development of periprosthetic infections after THA and TKA: a prospective matched-pair analysis of 240 patients.Clin Interv Aging. 2018 Aug 17;13:1429-1435. doi: 10.2147/CIA.S171307. eCollection 2018. Clin Interv Aging. 2018. PMID: 30147306 Free PMC article.
-
[Detection of malnutrition in geriatric trauma patients : A reassessment].Unfallchirurg. 2019 Nov;122(11):864-869. doi: 10.1007/s00113-018-0595-3. Unfallchirurg. 2019. PMID: 30607484 German.
-
Prevalence of Poor Nutrition in Knee Osteoarthritis Patients: A Hospital-Based Cohort Study in Indian Population.Indian J Orthop. 2024 Feb 4;58(3):298-307. doi: 10.1007/s43465-023-01090-3. eCollection 2024 Mar. Indian J Orthop. 2024. PMID: 38425822 Free PMC article.
-
[Lymphocyte Count, Serum Albumin and Transferrin Levels in Patients Undergoing Total Knee Arthroplasty].Rev Bras Ortop (Sao Paulo). 2025 Jul 25;60(2):1-11. doi: 10.1055/s-0045-1809530. eCollection 2025 Apr. Rev Bras Ortop (Sao Paulo). 2025. PMID: 40727702 Free PMC article. Portuguese.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
