

Clinical, biological, echocardiographic and therapeutic determinants of the length of hospital stay of patients with acute heart failure
- PMID: 24868258
- PMCID: PMC4034303
Clinical, biological, echocardiographic and therapeutic determinants of the length of hospital stay of patients with acute heart failure
Abstract
Hypothesis: The length of hospital stay (LOS) is a unanimously accepted measure of risk and treatment efficacy for in-patients.
Purpose: Our aim was to identify the parameters with predictive value for the LOS of patients with acute heart failure (AHF).
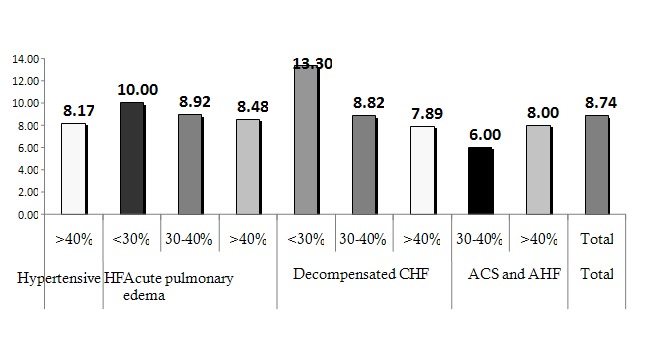
Methods: We analyzed 125 patients consecutively admitted to our clinic with a slight male predominance (54.4%) and a mean age of 71.54 years. Patients were divided into groups according to the clinical form at presentation and left ventricular function. Mean LOS was of 8.74 days.
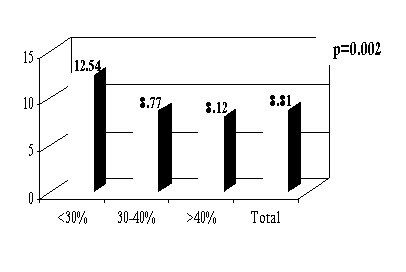
Results: Patients with LVEF<30% had a significantly higher LOS compared to those with LVEF>30% (F(2)=6.54, p<0.05). The same difference was discovered for those who received inotropic support (p<0.001), i.v. loop diuretic>140mg (p<0.001) as well as for those with QRS>160ms (p<0.05) or LBBB. The linear regression equation exposed a single significant statistical model indicating that the need for vasopressor amines, mean diuretic dose and PAAT<90msec explain 56% of the variance of LOS F(3.46)=20.55, p<0.001. The highest contribution to the model was achieved by the need for vasopressor amines (β=0.66), with a unique contribution of 42% to the variance of the number of days of stay. The mean dose of diuretic had β=0.27 and a unique contribution to the model of 7.2%, followed by PAAT<90 msec with β=0.26 and a unique contribution to the model of 7%.
Conclusions: LOS is influenced by numerous parameters, some specific to certain clinical forms of AHF while others are independent, which is why evaluations on larger groups of patients are further needed.
Keywords: LOS; acute heart failure; left ventricle ejection fraction; length of stay; pulmonary artery acceleration time.
Figures





References
-
- Hunt SA, Abraham WT, Chin MH. ACC/AHA 2005 Guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. . Circulation. 2005;112:154–235. - PubMed
-
- Thom T, Haase N, Rosamond W. Heart Disease and Stroke Statistics–2006 Update: a Report From the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113:85–151. - PubMed
-
- Felker GM, Adams KF, Konstam MA. The problem of decompensated heart failure: nomenclature, classification, and risk stratification. Am Heart J. 2003;145:S18–S25. - PubMed
-
- Butler J, Kalogeropoulos A. Worsening Heart Failure Hospitalization Epidemic We Do Not Know How to Prevent and We Do Not Know How to Treat!. J Am Coll Cardiol. 2008;52:435–437. - PubMed
-
- Keenan PS, Normand SL, Lin Z. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1:29–37. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous