

Pediatric lupus nephritis: Management update
- PMID: 24868499
- PMCID: PMC4023399
- DOI: 10.5527/wjn.v3.i2.16
Pediatric lupus nephritis: Management update
Abstract
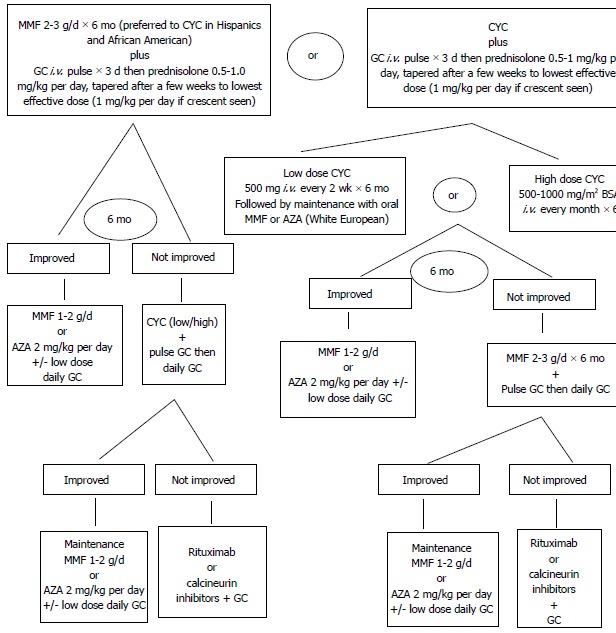
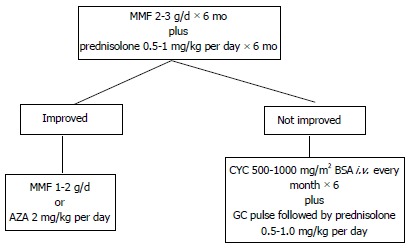
Childhood-onset systemic lupus erythematosus (cSLE) is a severe multisystem autoimmune disease. Renal involvement occurs in the majority of cSLE patients and is often fatal. Renal biopsy is an important investigation in the management of lupus nephritis. Treatment of renal lupus consists of an induction phase and maintenance phase. Treatment of childhood lupus nephritis using steroids is associated with poor outcome and excess side-effects. The addition of cyclophosphamide to the treatment schedule has improved disease control. In view of treatment failure using these drugs and a tendency for non-adherence, many newer agents such as immune-modulators and monoclonal antibodies are being tried in patients with cSLE. Trials of these novel agents in the pediatric population are still lacking making a consensus in the management protocol of pediatric lupus nephritis difficult.
Keywords: Cyclophosphamide; Lupus nephritis; Management; Monoclonal antibody; Mycophenolate mofetil; Pediatric.
Figures
References
-
- Kamphuis S, Silverman ED. Prevalence and burden of pediatric-onset systemic lupus erythematosus. Nat Rev Rheumatol. 2010;6:538–546. - PubMed
-
- Malleson PN, Fung MY, Rosenberg AM. The incidence of pediatric rheumatic diseases: results from the Canadian Pediatric Rheumatology Association Disease Registry. J Rheumatol. 1996;23:1981–1987. - PubMed
-
- Huang JL, Yao TC, See LC. Prevalence of pediatric systemic lupus erythematosus and juvenile chronic arthritis in a Chinese population: a nation-wide prospective population-based study in Taiwan. Clin Exp Rheumatol. 2004;22:776–780. - PubMed
-
- Baqi N, Moazami S, Singh A, Ahmad H, Balachandra S, Tejani A. Lupus nephritis in children: a longitudinal study of prognostic factors and therapy. J Am Soc Nephrol. 1996;7:924–929. - PubMed
-
- Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40:1725. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
