

Improved survival with T cell clonotype stability after anti-CTLA-4 treatment in cancer patients
- PMID: 24871131
- PMCID: PMC4558099
- DOI: 10.1126/scitranslmed.3008211
Improved survival with T cell clonotype stability after anti-CTLA-4 treatment in cancer patients
Abstract
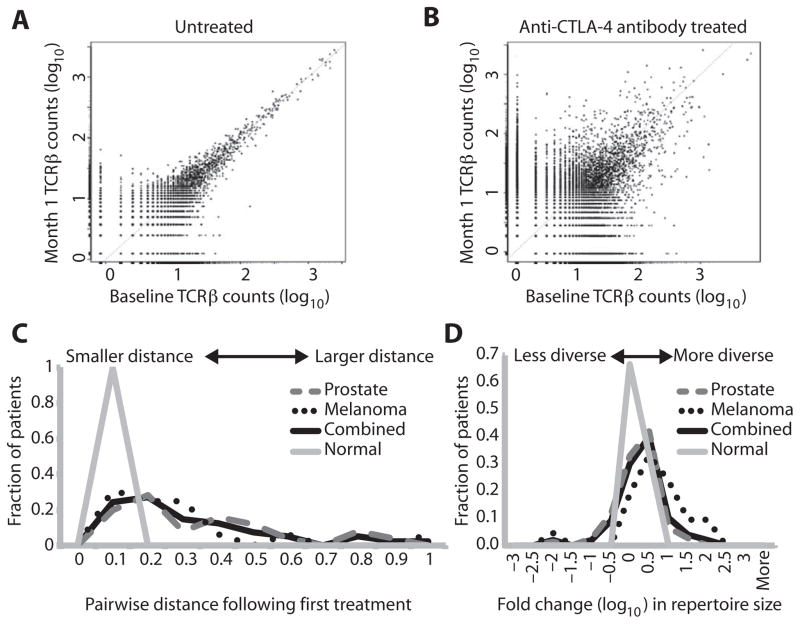
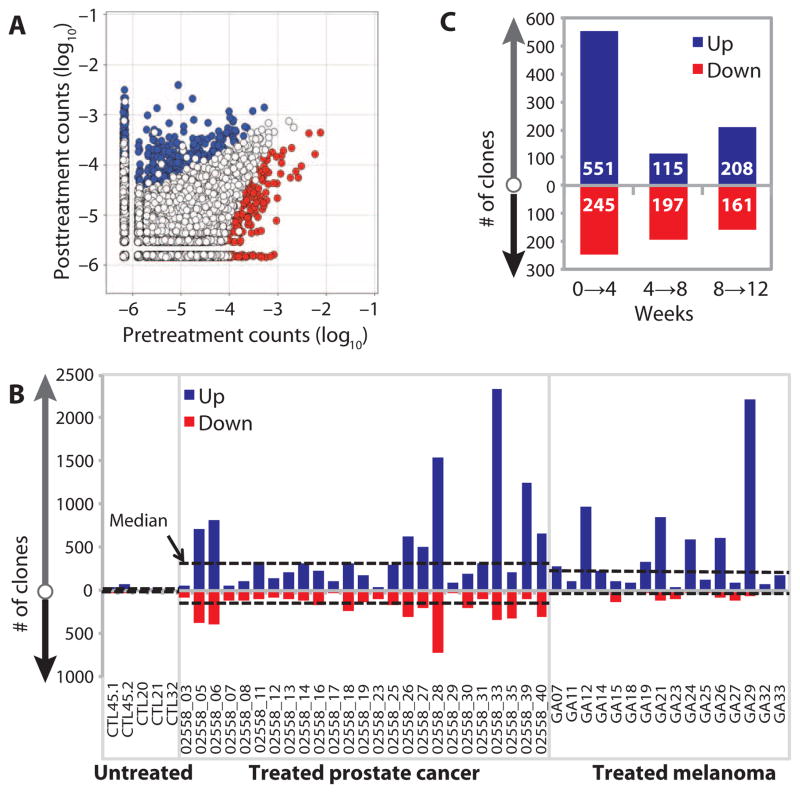
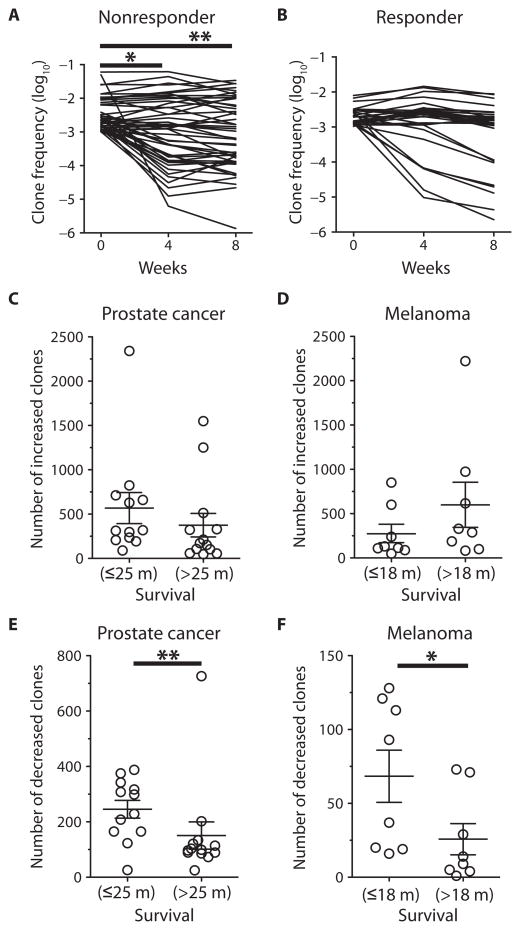
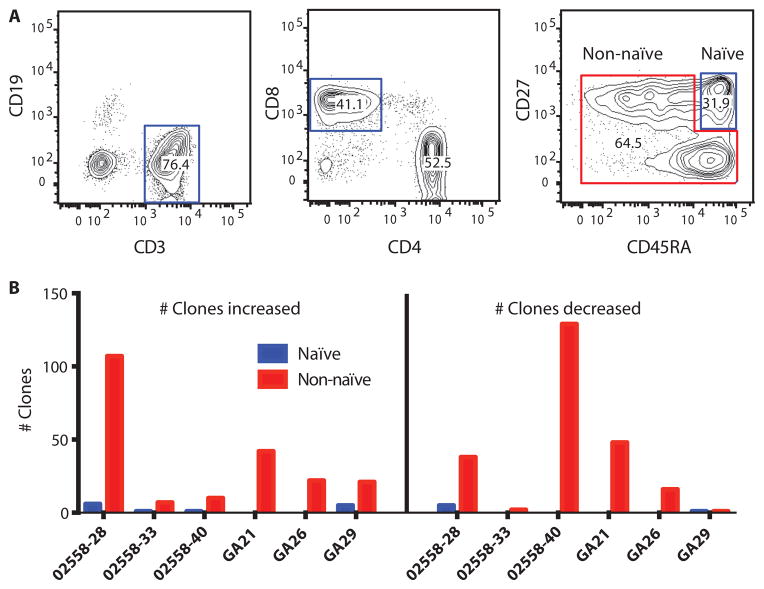
Cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) blockade can promote antitumor T cell immunity and clinical responses. The mechanism by which anti-CTLA-4 antibodies induces antitumor responses is controversial. To determine the effects of CTLA-4 blockade on the T cell repertoire, we used next-generation deep sequencing to measure the frequency of individual rearranged T cell receptor β (TCRβ) genes, thereby characterizing the diversity of rearrangements, known as T cell clonotypes. CTLA-4 blockade in patients with metastatic castration-resistant prostate cancer and metastatic melanoma resulted in both expansion and loss of T cell clonotypes, consistent with a global turnover of the T cell repertoire. Overall, this treatment increased TCR diversity as reflected in the number of unique TCR clonotypes. The repertoire of clonotypes continued to evolve over subsequent months of treatment. Whereas the number of clonotypes that increased with treatment was not associated with clinical outcome, improved overall survival was associated with maintenance of high-frequency clones at baseline. In contrast, the highest-frequency clonotypes fell with treatment in patients with short overall survival. Stably maintained clonotypes included T cells having high-avidity TCR such as virus-reactive T cells. Together, these results suggest that CTLA-4 blockade induces T cell repertoire evolution and diversification. Moreover, improved clinical outcomes are associated with less clonotype loss, consistent with the maintenance of high-frequency TCR clonotypes during treatment. These clones may represent the presence of preexisting high-avidity T cells that may be relevant in the antitumor response.
Copyright © 2014, American Association for the Advancement of Science.
Conflict of interest statement
Figures
References
-
- Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science. 1996;271:1734–1736. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
