

Defining the clinical course of multiple sclerosis: the 2013 revisions
- PMID: 24871874
- PMCID: PMC4117366
- DOI: 10.1212/WNL.0000000000000560
Defining the clinical course of multiple sclerosis: the 2013 revisions
Abstract
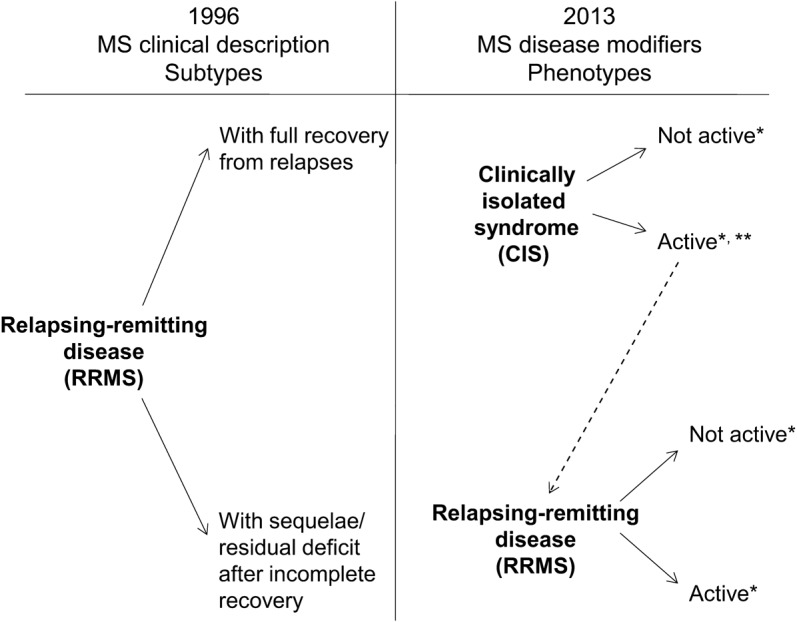
Accurate clinical course descriptions (phenotypes) of multiple sclerosis (MS) are important for communication, prognostication, design and recruitment of clinical trials, and treatment decision-making. Standardized descriptions published in 1996 based on a survey of international MS experts provided purely clinical phenotypes based on data and consensus at that time, but imaging and biological correlates were lacking. Increased understanding of MS and its pathology, coupled with general concern that the original descriptors may not adequately reflect more recently identified clinical aspects of the disease, prompted a re-examination of MS disease phenotypes by the International Advisory Committee on Clinical Trials of MS. While imaging and biological markers that might provide objective criteria for separating clinical phenotypes are lacking, we propose refined descriptors that include consideration of disease activity (based on clinical relapse rate and imaging findings) and disease progression. Strategies for future research to better define phenotypes are also outlined.
© 2014 American Academy of Neurology.
Figures

Comment in
-
Active and progressive: a new duality of MS classification.Neurology. 2014 Jul 15;83(3):206-7. doi: 10.1212/WNL.0000000000000601. Epub 2014 Jun 13. Neurology. 2014. PMID: 24928117 No abstract available.
-
Defining the clinical course of multiple sclerosis: the 2013 revisions.Neurology. 2015 Mar 3;84(9):963. doi: 10.1212/01.wnl.0000462309.76486.c5. Neurology. 2015. PMID: 25732366 No abstract available.
-
Author response.Neurology. 2015 Mar 3;84(9):963. Neurology. 2015. PMID: 25905117 No abstract available.
References
-
- Lublin FD, Reingold SC. Defining the clinical course of multiple sclerosis: results of an international survey. Neurology 1996;46:907–911 - PubMed
-
- Miller D, Barkhof F, Montalban X, Thompson A, Filippi M. Clinically isolated syndromes suggestive of multiple sclerosis, part I: natural history, pathogenesis, diagnosis, and prognosis. Lancet Neurol 2005;4:281–288 - PubMed
-
- O'Riordan JI, Thompson AJ, Kingsley DP, et al. The prognostic value of brain MRI in clinically isolated syndromes of the CNS: a 10-year follow-up. Brain 1998;121:495–503 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical