

Increased 1-year healthcare use in survivors of severe sepsis
- PMID: 24872085
- PMCID: PMC4226030
- DOI: 10.1164/rccm.201403-0471OC
Increased 1-year healthcare use in survivors of severe sepsis
Abstract
Rationale: Hospitalizations for severe sepsis are common, and a growing number of patients survive to hospital discharge. Nonetheless, little is known about survivors' post-discharge healthcare use.
Objectives: To measure inpatient healthcare use of severe sepsis survivors compared with patients' own presepsis resource use and the resource use of survivors of otherwise similar nonsepsis hospitalizations.
Methods: This is an observational cohort study of survivors of severe sepsis and nonsepsis hospitalizations identified from participants in the Health and Retirement Study with linked Medicare claims, 1998-2005. We matched severe sepsis and nonsepsis hospitalizations by demographics, comorbidity burden, premorbid disability, hospitalization length, and intensive care use.
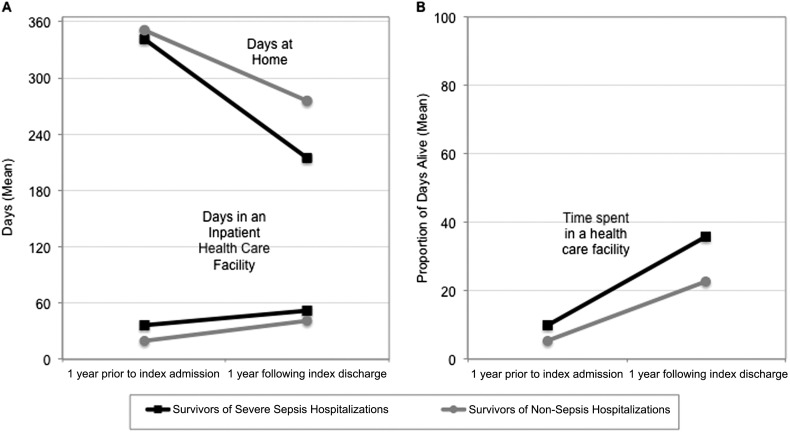
Measurements and main results: Using Medicare claims, we measured patients' use of inpatient facilities (hospitals, long-term acute care hospitals, and skilled nursing facilities) in the 2 years surrounding hospitalization. Severe sepsis survivors spent more days (median, 16 [interquartile range, 3-45] vs. 7 [0-29]; P < 0.001) and a higher proportion of days alive (median, 9.6% [interquartile range, 1.4-33.8%] vs. 1.9% [0.0-7.9%]; P < 0.001) admitted to facilities in the year after hospitalization, compared with the year prior. The increase in facility-days was similar for nonsepsis hospitalizations. However, the severe sepsis cohort experienced greater post-discharge mortality (44.2% [95% confidence interval, 41.3-47.2%] vs. 31.4% [95% confidence interval, 28.6-34.2%] at 1 year), a steeper decline in days spent at home (difference-in-differences, -38.6 d [95% confidence interval, -50.9 to 26.3]; P < 0.001), and a greater increase in the proportion of days alive spent in a facility (difference-in-differences, 5.4% [95% confidence interval, 2.8-8.1%]; P < 0.001).
Conclusions: Healthcare use is markedly elevated after severe sepsis, and post-discharge management may be an opportunity to reduce resource use.
Keywords: healthcare facilities; hospitalization; patient outcomes assessment; patient readmission; skilled nursing facility.
Figures


Comment in
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Kumar G, Kumar N, Taneja A, Kaleekal T, Tarima S, McGinley E, Jimenez E, Mohan A, Khan RA, Whittle J, et al. Milwaukee Initiative in Critical Care Outcomes Research Group of Investigators. Nationwide trends of severe sepsis in the 21st century (2000-2007) Chest. 2011;140:1223–1231. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- Quartin AA, Schein RM, Kett DH, Peduzzi PN Department of Veterans Affairs Systemic Sepsis Cooperative Studies Group. Magnitude and duration of the effect of sepsis on survival. JAMA. 1997;277:1058–1063. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
