

Impact and programmatic implications of routine viral load monitoring in Swaziland
- PMID: 24872139
- PMCID: PMC4149657
- DOI: 10.1097/QAI.0000000000000224
Impact and programmatic implications of routine viral load monitoring in Swaziland
Abstract
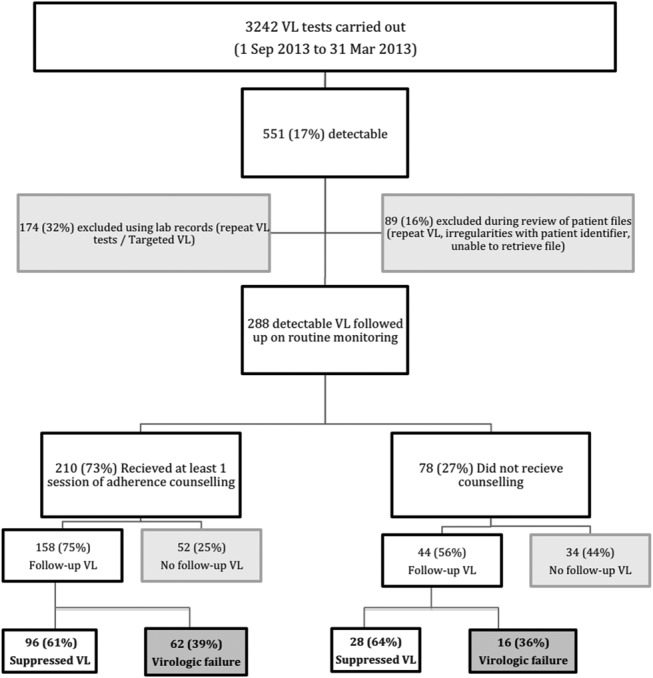
Objective: To assess the programmatic quality (coverage of testing, counseling, and retesting), cost, and outcomes (viral suppression, treatment decisions) of routine viral load (VL) monitoring in Swaziland.
Design: Retrospective cohort study of patients undergoing routine VL monitoring in Swaziland (October 1, 2012 to March 31, 2013).
Results: Of 5563 patients eligible for routine VL testing monitoring in the period of study, an estimated 4767 patients (86%) underwent testing that year. Of 288 patients with detectable VL, 210 (73%) underwent enhanced adherence counseling and 202 (70%) had a follow-up VL within 6 months. Testing coverage was slightly lower in children, but coverage of retesting was similar between and age groups and sexes. Of those with a follow-up test, 126 (62%) showed viral suppression. The remaining 78 patients had World Health Organization-defined virologic failure; 41 (53%) were referred by the doctor for more adherence counseling, and 13 (15%) were changed to second-line therapy, equating to an estimated rate of 1.2 switches per 100 patient-years. Twenty-four patients (32%) were transferred out, lost to follow-up, or not reviewed by doctor. The "fully loaded" cost of VL monitoring was $35 per patient-year.
Conclusions: Achieving good quality VL monitoring is feasible and affordable in resource-limited settings, although close supervision is needed to ensure good coverage of testing and counseling. The low rate of switch to second-line therapy in patients with World Health Organization-defined virologic failure seems to reflect clinician suspicion of ongoing adherence problems. In our study, the main impact of routine VL monitoring was reinforcing adherence rather than increasing use of second-line therapy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- WHO. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection. Recommendations for a Public Health Approach. World Health Organization, Geneva, 2013 - PubMed
-
- Kunutsor S, Walley J, Muchuro S, et al. Improving adherence to antiretroviral therapy in sub-Saharan African HIV-positive populations: an enhanced adherence package. AIDS Care. 2012;24:1308–1315 - PubMed
-
- Sigaloff KCE, Hamers RL, Wallis CL, et al. Unnecessary antiretroviral treatment switches and accumulation of HIV resistance mutations; two arguments for viral load monitoring in Africa. J Acquir Immune Defic Syndr. 2011;58:23–31 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
