Prevalence of Chronic Mountain Sickness in high altitude districts of Himachal Pradesh
- PMID: 24872667
- PMCID: PMC4035612
- DOI: 10.4103/0019-5278.130839
Prevalence of Chronic Mountain Sickness in high altitude districts of Himachal Pradesh
Abstract
Introduction: Chronic Mountain Sickness (CMS) is a maladaptation condition that can affect people who reside permanently at high altitude (HA). It is characterized by polycythemia, hypoxemia and dyspnea and can be fatal. Over 140 million people live permanently at HA around the world. Unfortunately, research into CMS is lacking and accurate data on the prevalence of this condition do not exist for many regions around the world. In this study, we sought to examine prevalence rates of CMS in the Indian Himalayas, focusing on the Northern State of Himachal Pradesh.
Materials and methods: We surveyed 83 individuals (69 males) in eight towns across the HA districts of Sirmaur, Kinnaur and Lahaul and Spiti in Himachal Pradesh, India. Altitudes ranged from 2350 to 4150 m. We used an adapted Qinghai CMS scoring system to diagnose CMS. Information related to subject demographics, medical history, socioeconomic status, and geography were collected to identify risk factors for CMS. Physiologic recordings of oxygen saturation (SpO2) and pulse rate were made through pulse oximetry.
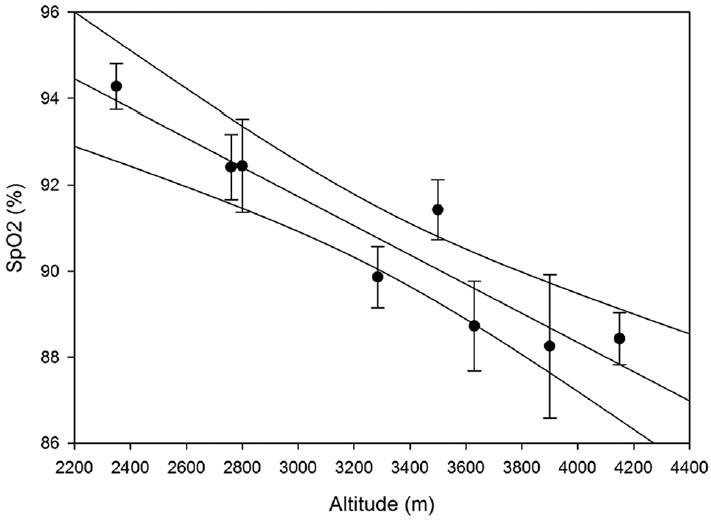
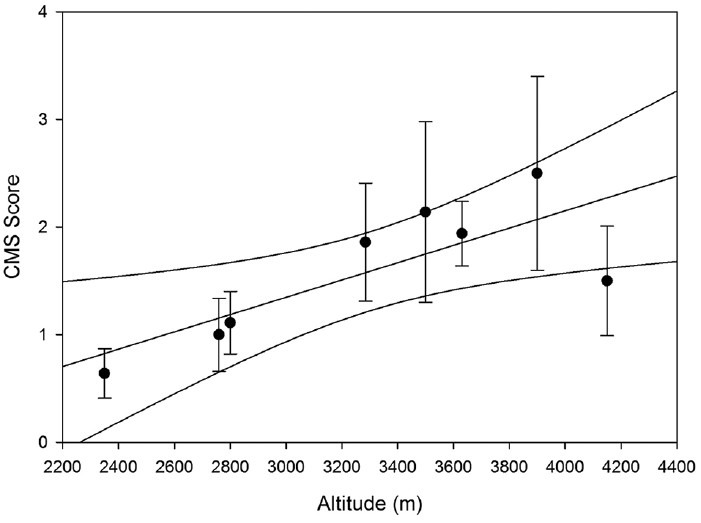
Results: Overall CMS prevalence was 6.17% and mean altitude was 3281 m. At altitudes above 3000 m CMS prevalence rose to 13.73%. All cases of CMS were mild and there was a significant positive correlation between CMS scores and altitude (R = 0.784, P = 0.0213). Mean SpO2 was 90.7 ± 0.4% and mean pulse rate was 80.3 ± 1.3 bpm. SpO2 significantly correlated with altitude (R = -0.929, P < 0.001). In our study, age, gender, and tobacco use were not independent risk factors for CMS. Individuals with CMS lived at higher altitudes than their non-CMS counterparts (3736.00 ± 113.30 m vs. 3279.80 ± 69.50 m, respectively; P = 0.017).
Conclusion: CMS prevalence in HA towns of the Indian Himalayas of Himachal Pradesh is 6.17% and 13.73% for towns above 3000 m. Further research is required to determine the prevalence of CMS in other regions of the world and to determine risk factors associated with CMS.
Keywords: Altitude physiology; Himalayas; chronic mountain sickness; environmental physiology; epidemiology; hypoxia.
Conflict of interest statement
Figures
References
-
- Penaloza D, Arias-Stella J. The heart and pulmonary circulation at high altitudes: Healthy highlanders and chronic mountain sickness. Circulation. 2007;115:1132–46. - PubMed
-
- León-Velarde F, Maggiorini M, Reeves JT, Aldashev A, Asmus I, Bernardi L, et al. Consensus statement on chronic and subacute high altitude diseases. High Alt Med Biol. 2005;6:147–57. - PubMed
-
- Pasha MA, Newman JH. High-altitude disorders: Pulmonary hypertension: Pulmonary vascular disease: The global perspective. Chest. 2010;137(6 Suppl):13S–9. - PubMed
-
- Rivera-Ch M, León-Velarde F, Huicho L. Treatment of chronic mountain sickness: Critical reappraisal of an old problem. Respir Physiol Neurobiol. 2007;158:251–65. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources