

The forehead flap: the gold standard of nasal soft tissue reconstruction
- PMID: 24872749
- PMCID: PMC3743909
- DOI: 10.1055/s-0033-1351231
The forehead flap: the gold standard of nasal soft tissue reconstruction
Abstract
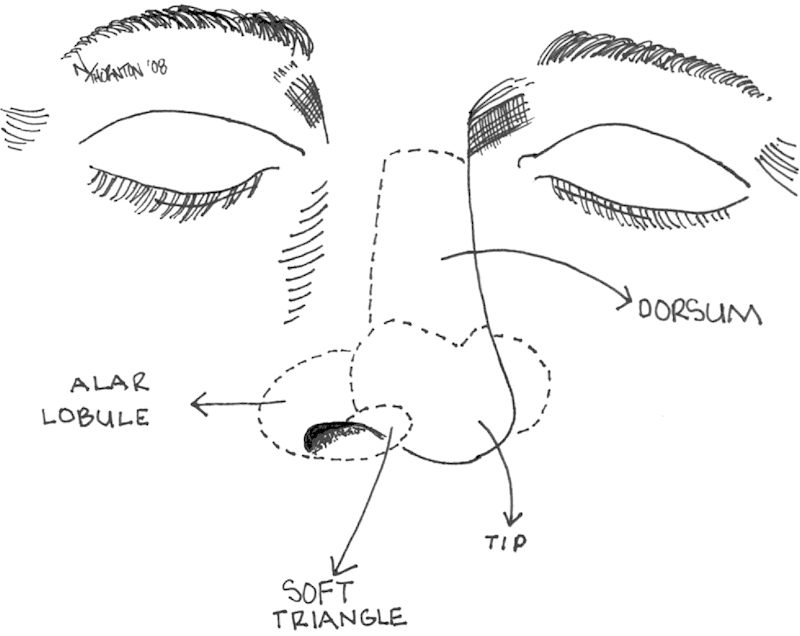
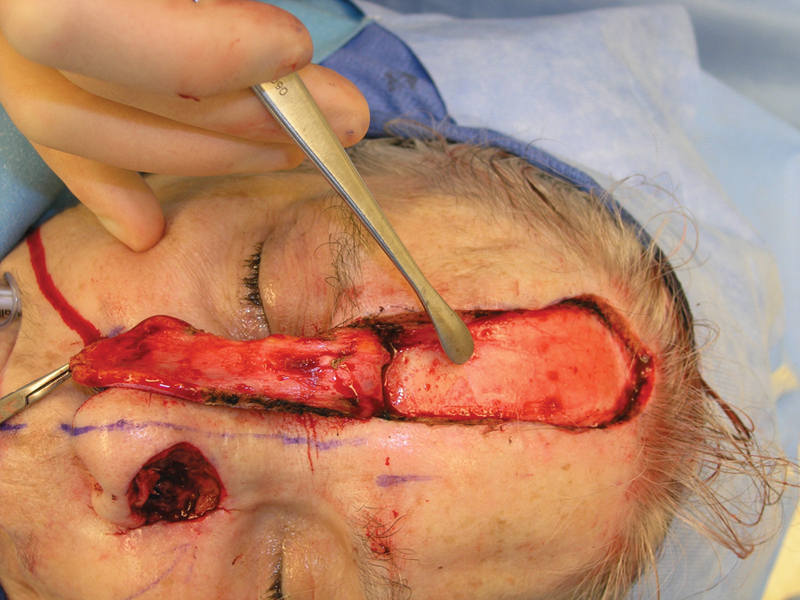
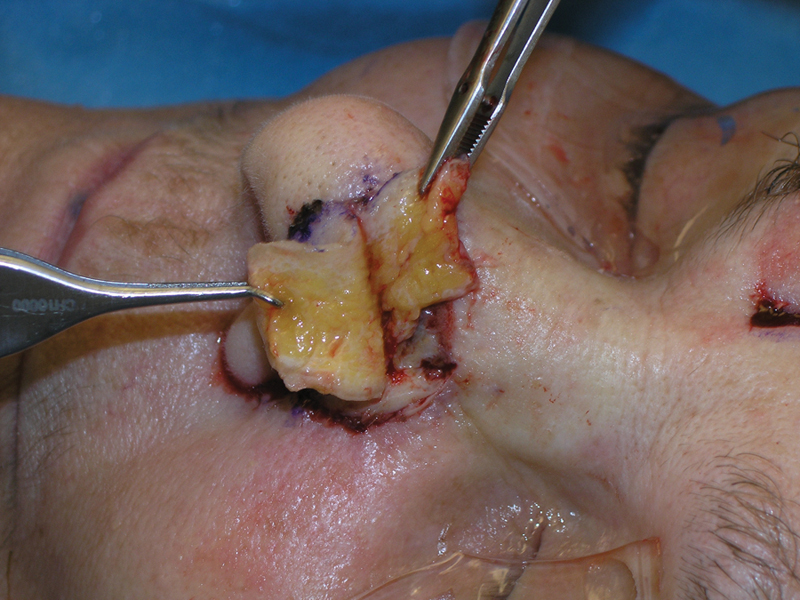
The forehead flap is one of the oldest recorded surgical techniques for nasal reconstruction. As the gold standard for nasal soft tissue reconstruction, the forehead flap provides a reconstructive surgeon with a robust pedicle and large amount of tissue to reconstruct almost any defect. Modifications provided by masters like Burget and Menick have only increased the utility of this exceptional flap. Maintaining an axial pattern, utilizing the pedicle ipsilateral to the defect, extending the flap at right angles with caution when extra length is needed, using a narrow pedicle, and early subperiosteal dissection are the guiding principles for forehead flap reconstruction of the nose. In addition, lining defects can be addressed simply and reliably with a folded forehead flap.
Keywords: Mohs surgery; forehead flap; nasal lining; nasal reconstruction.
Figures








References
-
- Converse J M. Philadelphia, Pa: WB Saunders; 1964. Reconstructive Plastic Surgery; p. 797.
-
- Conley J J, Price J C. The midline vertical forehead flap. Otolaryngol Head Neck Surg. 1981;89(1):38–44. - PubMed
-
- Converse J M. Philadelphia, PA: WB Saunders; 1977. Reconstructive Plastic Surgery. 2nd ed; p. 694.
-
- Jackson I T. St. Louis, MO: Mosby; 1985. Local Flaps in Head and Neck Reconstruction.
-
- Burget G C, Menick F J. Nasal support and lining: the marriage of beauty and blood supply. Plast Reconstr Surg. 1989;84(2):189–202. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
