

Robotic-assisted latissimus dorsi harvest in delayed-immediate breast reconstruction
- PMID: 24872775
- PMCID: PMC3946018
- DOI: 10.1055/s-0034-1368163
Robotic-assisted latissimus dorsi harvest in delayed-immediate breast reconstruction
Abstract
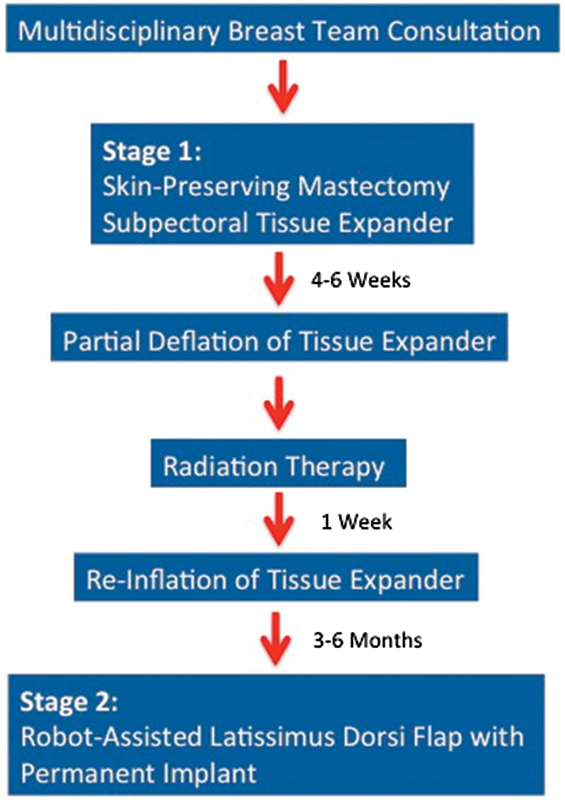
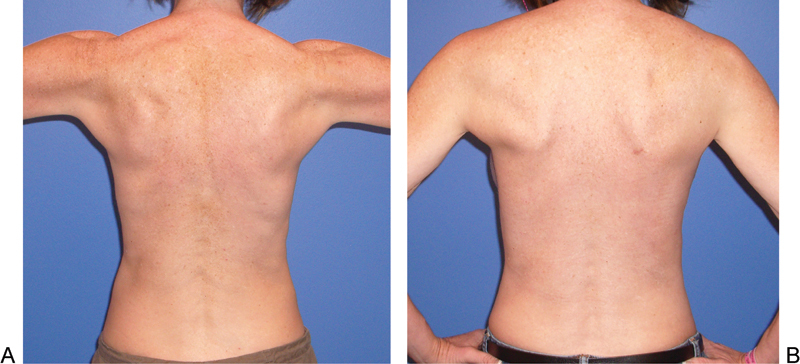
For two-stage, implant-based, delayed-immediate reconstruction of the radiated breast, robotic-assisted latissimus dorsi harvest (RALDH) is a good option for patients who wish to avoid a traditional latissimus dorsi donor-site incision. The purpose of this study was to compare outcomes of RALDH and the traditional open technique (TOT) for patients undergoing delayed-immediate breast reconstruction following radiation therapy. A retrospective analysis of a prospective database of all consecutive patients undergoing latissimus dorsi harvest for radiated breast reconstruction between 2009 and 2013 was performed. Indications, surgical technique, complications, and outcomes were assessed. One hundred forty-six pedicled latissimus dorsi muscle flaps were performed for breast reconstruction and 17 were performed robotically during the study period (average follow-up 14.6 ± 7.3 mo). Latissimus dorsi breast reconstruction following radiation was performed in 64 patients using TOT and 12 using RALDH. Surgical complication rates were 37.5% in TOT versus 16.7% in RALDH (p = 0.31) including seroma (8.9% versus 8.3%), infection (14.1 versus 8.3%), delayed wound healing (7.8% versus 0), and capsular contracture (4.7% vs. 0). Robotic-assisted harvest of the latissimus dorsi muscle is associated with a low complication rate and reliable results for delayed reconstruction of the irradiated breast while eliminating the need for a donor-site incision.
Keywords: breast reconstruction; delayed immediate; latissimus dorsi; radiated breast; robotic assisted.
Figures

Similar articles
-
Robotic-assisted harvest of latissimus dorsi muscle flap for breast reconstruction: review of the literature.J Robot Surg. 2022 Feb;16(1):15-19. doi: 10.1007/s11701-021-01232-5. Epub 2021 Mar 23. J Robot Surg. 2022. PMID: 33755925 Review.
-
Comparing Outcomes of Robotically Assisted Latissimus Dorsi Harvest to the Traditional Open Approach in Breast Reconstruction.Plast Reconstr Surg. 2020 Dec;146(6):1221-1225. doi: 10.1097/PRS.0000000000007368. Plast Reconstr Surg. 2020. PMID: 33234946
-
Outcomes of delayed abdominal-based autologous reconstruction versus latissimus dorsi flap plus implant reconstruction in previously irradiated patients.Ann Plast Surg. 2012 Oct;69(4):380-2. doi: 10.1097/SAP.0b013e31824b3d6b. Ann Plast Surg. 2012. PMID: 22964681
-
Robotic latissimus dorsi muscle harvest: a case series.Plast Reconstr Surg. 2012 Jun;129(6):1305-1312. doi: 10.1097/PRS.0b013e31824ecc0b. Plast Reconstr Surg. 2012. PMID: 22634647
-
The Present and Future of Robotic Surgery in Breast Cancer and Breast Reconstruction.J Clin Med. 2025 Mar 19;14(6):2100. doi: 10.3390/jcm14062100. J Clin Med. 2025. PMID: 40142908 Free PMC article. Review.
Cited by
-
Robotic-assisted harvest of latissimus dorsi muscle flap for breast reconstruction: review of the literature.J Robot Surg. 2022 Feb;16(1):15-19. doi: 10.1007/s11701-021-01232-5. Epub 2021 Mar 23. J Robot Surg. 2022. PMID: 33755925 Review.
-
Robotic-Assisted Microsurgery and Its Future in Plastic Surgery.J Clin Med. 2022 Jun 13;11(12):3378. doi: 10.3390/jcm11123378. J Clin Med. 2022. PMID: 35743450 Free PMC article. Review.
-
Six steps for a successful aesthetic free flap reconstruction after minimally invasive mastectomy: a retrospective case-control study.Int J Surg. 2024 Feb 1;110(2):645-653. doi: 10.1097/JS9.0000000000000871. Int J Surg. 2024. PMID: 38000051 Free PMC article.
-
Robotic omental flap harvest for near-total anterior chest wall coverage: a potential application of robotic techniques in plastic and reconstructive surgery.BMJ Case Rep. 2021 Feb 23;14(2):e237887. doi: 10.1136/bcr-2020-237887. BMJ Case Rep. 2021. PMID: 33622742 Free PMC article.
-
Robotic-Assisted Nipple Sparing Mastectomy.Semin Plast Surg. 2023 Jul 17;37(3):176-183. doi: 10.1055/s-0043-1771047. eCollection 2023 Aug. Semin Plast Surg. 2023. PMID: 38444956 Free PMC article. Review.
References
-
- Ascherman J A, Hanasono M M, Newman M I, Hughes D B. Implant reconstruction in breast cancer patients treated with radiation therapy. Plast Reconstr Surg. 2006;117(2):359–365. - PubMed
-
- Spear S L, Onyewu C. Staged breast reconstruction with saline-filled implants in the irradiated breast: recent trends and therapeutic implications. Plast Reconstr Surg. 2000;105(3):930–942. - PubMed
-
- Kronowitz S J, Robb G L. Radiation therapy and breast reconstruction: a critical review of the literature. Plast Reconstr Surg. 2009;124(2):395–408. - PubMed
-
- Tran N V, Chang D W, Gupta A, Kroll S S, Robb G L. Comparison of immediate and delayed free TRAM flap breast reconstruction in patients receiving postmastectomy radiation therapy. Plast Reconstr Surg. 2001;108(1):78–82. - PubMed
-
- Spear S L, Boehmler, Clemens M W The latissimus flap in the irradiated breast Philadelphia, PA: Lippincott-Raven; 2011563–570.
LinkOut - more resources
Full Text Sources
Other Literature Sources
