

Davunetide in patients with progressive supranuclear palsy: a randomised, double-blind, placebo-controlled phase 2/3 trial
- PMID: 24873720
- PMCID: PMC4129545
- DOI: 10.1016/S1474-4422(14)70088-2
Davunetide in patients with progressive supranuclear palsy: a randomised, double-blind, placebo-controlled phase 2/3 trial
Abstract
Background: In preclinical studies, davunetide promoted microtubule stability and reduced tau phosphorylation. Because progressive supranuclear palsy (PSP) is linked to tau pathology, davunetide could be a treatment for PSP. We assessed the safety and efficacy of davunetide in patients with PSP.
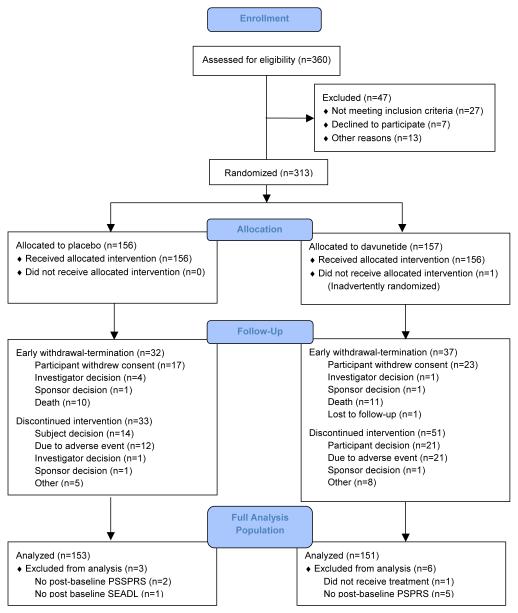
Methods: In a double-blind, parallel group, phase 2/3 trial, participants were randomly assigned with permuted blocks in a 1:1 ratio to davunetide (30 mg twice daily, intranasally) or placebo for 52 weeks at 48 centres in Australia, Canada, France, Germany, the UK, and the USA. Participants met the modified Neuroprotection and Natural History in Parkinson Plus Syndrome study criteria for PSP. Primary endpoints were the change from baseline in PSP Rating Scale (PSPRS) and Schwab and England Activities of Daily Living (SEADL) scale at up to 52 weeks. All participants and study personnel were masked to treatment assignment. Analysis was by intention to treat. The trial is registered with Clinicaltrials.gov, number NCT01110720.
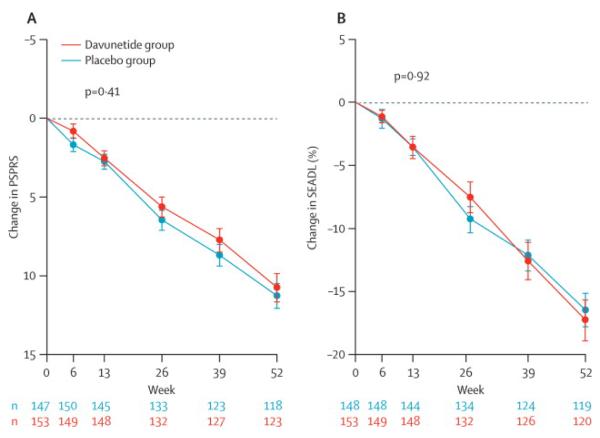
Findings: 313 participants were randomly assigned to davunetide (n=157) or to placebo (n=156), and 241 (77%) completed the study (118 and 156 in the davunetide and placebo groups, respectively). There were no differences in the davunetide and placebo groups in the baseline PSPRS and SEADL. The davunetide and placebo groups did not differ in the change from baseline in PSPRS (median 11·8 [95% CI 10·5 to 13·0] vs 11·8 [10·5 to 13·0], respectively, p=0·41) or SEADL (-0·20 [-0·20 to -0·17] vs -0·20 [-0·22 to -0·17], respectively, p=0·92). 54 serious adverse events were reported in each of the treatment groups, including 11 deaths in the davunetide group and ten in the placebo group. The frequency of nasal adverse events was greater in the davunetide group than in the placebo group (epistaxis 18 [12%] of 156 vs 13 [8%] of 156, rhinorrhoea 15 [10%] vs eight [5%], and nasal discomfort 15 [10%] vs one [<1%]).
Interpretation: Davunetide is not an effective treatment for PSP. Clinical trials of disease-modifying treatment are feasible in patients with PSP and should be pursued with other promising tau-directed treatments.
Funding: Allon Therapeutics.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
When should neuroprotective drugs move from mice to men?Lancet Neurol. 2014 Jul;13(7):641-3. doi: 10.1016/S1474-4422(14)70112-7. Epub 2014 May 27. Lancet Neurol. 2014. PMID: 24873721 No abstract available.
References
-
- Stamelou M, de Silva R, Arias-Carrion O, et al. Rational therapeutic approaches to progressive supranuclear palsy. Brain. 2010;133(Pt 6):1578–90. - PubMed
-
- Steele JC, Richardson JC, Olszewski J, Progressive Supranuclear Palsy A Heterogeneous Degeneration Involving the Brain Stem, Basal Ganglia and Cerebellum with Vertical Gaze and Pseudobulbar Palsy, Nuchal Dystonia and Dementia. Arch Neurol. 1964;10:333–59. - PubMed
-
- Williams DR, Lees AJ. Progressive supranuclear palsy: clinicopathological concepts and diagnostic challenges. Lancet Neurol. 2009;8(3):270–9. - PubMed
-
- Nath U, Ben-Shlomo Y, Thomson RG, et al. The prevalence of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome) in the UK. Brain. 2001;124(Pt 7):1438–49. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
