

Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction
- PMID: 24874200
- PMCID: PMC4102617
- DOI: 10.1161/CIRCHEARTFAILURE.113.001281
Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction
Abstract
Background: Hospitalization for acute heart failure (HF) is associated with high rates of subsequent mortality and readmission. We assessed the influence of the time interval between previous HF hospitalization and randomization in the Candesartan in Heart failure: Reduction in Mortality and morbidity (CHARM) trials on clinical outcomes in patients with both reduced and preserved ejection fraction.
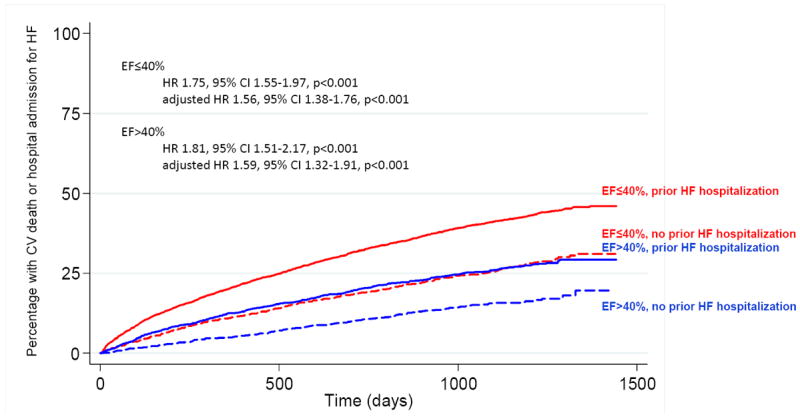
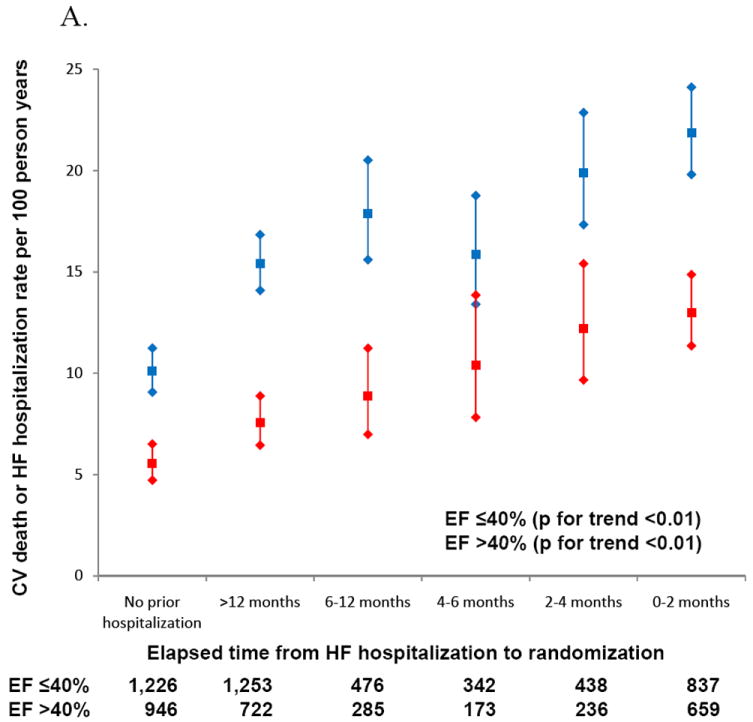
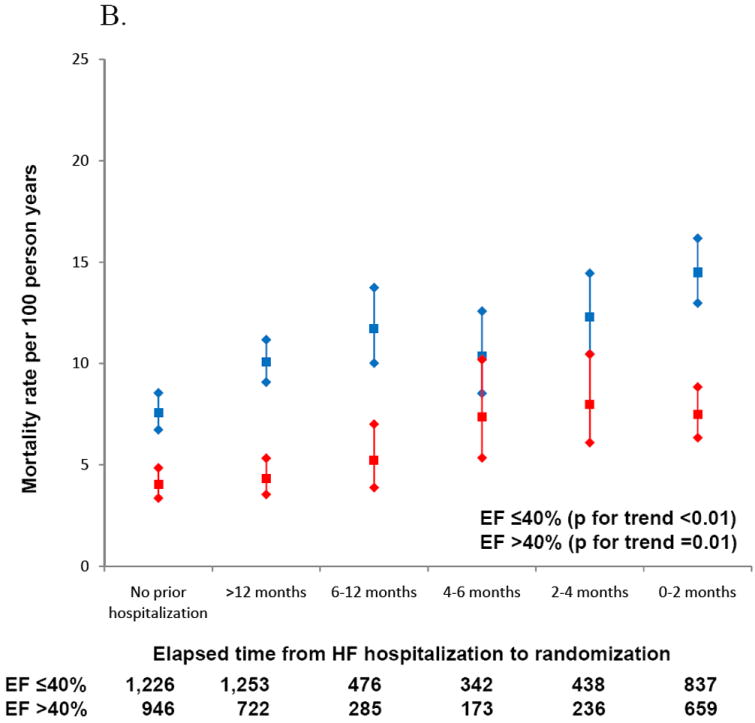
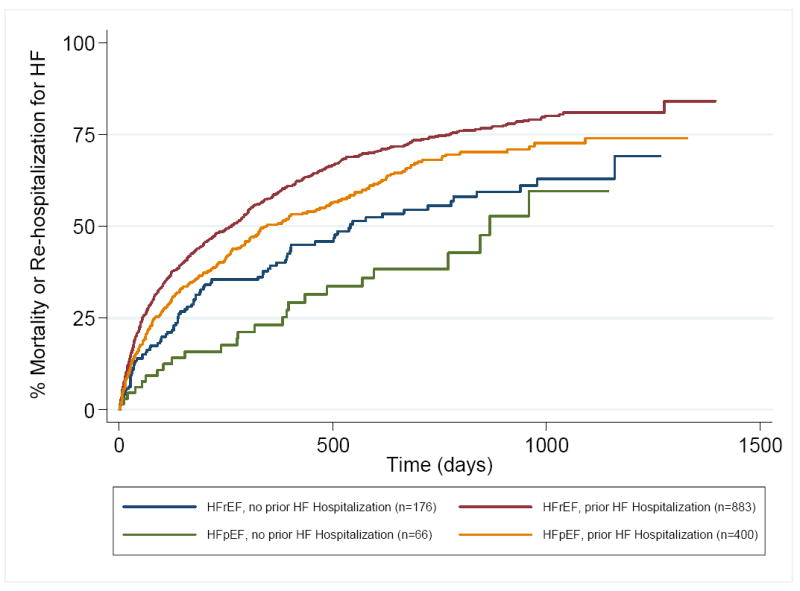
Methods and results: CHARM enrolled 7599 patients with New York Heart Association class II to IV HF, of whom 5426 had a history of previous HF hospitalization. Cox proportional hazards regression models were used to assess the association between time from previous HF hospitalization and randomization and the primary outcome of cardiovascular death or unplanned admission to hospital for the management of worsening HF during a median of 36.6 months. For patients with HF and reduced or preserved ejection fraction, rates of cardiovascular mortality and HF hospitalization were higher among patients with previous HF hospitalization than those without. The risk for mortality and hospitalization varied inversely with the time interval between hospitalization and randomization. Rates were higher for patients with HF and reduced ejection fraction within each category. Event rates for those with HF with preserved ejection fraction and a HF hospitalization in the 6 months before randomization were comparable with the rate in patients with HF and reduced ejection fraction with no previous HF hospitalization.
Conclusions: Rates of cardiovascular death or HF hospitalization are greatest in those who have been previously hospitalized for HF. Independent of EF, rates of death and readmission decline as time from HF hospitalization to trial enrollment increased. Recent HF hospitalization identifies a high-risk population for future clinical trials in HF and reduced ejection fraction and HF with preserved ejection fraction.
Clinical trial registration url: http://www.clinicaltrials.gov. Unique identifier: NCT00634400.
Keywords: clinical trials; heart failure; hospitalization; outcomes assessment.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Drs. Desai, Claggett, and Bello report no conflicts.
Figures
References
-
- Solomon SD, Dobson J, Pocock S, Skali H, McMurray JJ, Granger CB, Yusuf S, Swedberg K, Young JB, Michelson EL, Pfeffer MA. Influence of nonfatal hospitalization for heart failure on subsequent mortality in patients with chronic heart failure. Circulation. 2007;116:1482–7. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of Heart Failure with Preserved Ejection Fraction in a Population-Based Study. N Engl J Med. 2006;355:260–9. - PubMed
-
- Cowie MR, Mosterd A, Wood DA, Deckers JW, Poole-Wilson PA, Sutton GC, Sutton GC, Grobbee DE. The epidemiology of heart failure. Eur Heart J. 1997;18:208–25. - PubMed
-
- Krumholz HM, Chen J, Murillo JE, Cohen DJ, Radford MJ. Admission to hospitals with onsite cardiac catheterization facilities :impact on long-term costs and outcomes. Circulation. 1998;98:2010–6. - PubMed
-
- Roguin A, Behar D, Ben Ami H, Reisner SA, Edelstein S, Linn S, Edoute Y. Long-term prognosis of acute pulmonary oedema--an ominous outcome. Eur J Heart Fail. 2000;2:137–44. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
