

Enhancing brain lesions after endovascular treatment of aneurysms
- PMID: 24874528
- PMCID: PMC7966257
- DOI: 10.3174/ajnr.A3976
Enhancing brain lesions after endovascular treatment of aneurysms
Abstract
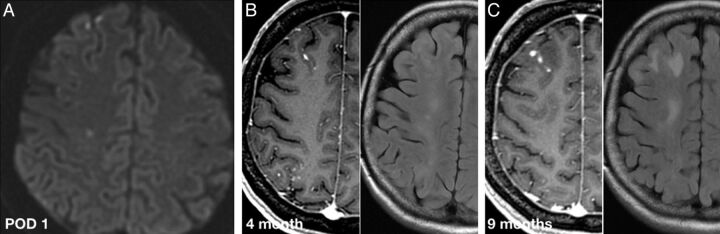
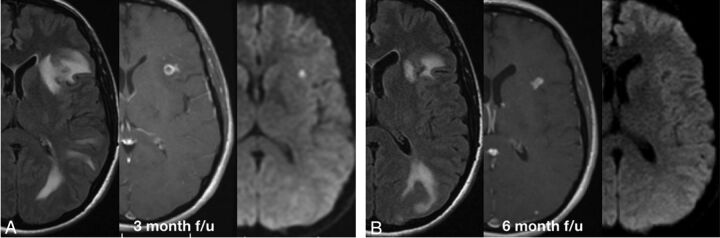
Complications of endovascular therapy of aneurysms mainly include aneurysm rupture and thromboembolic events. The widespread use of MR imaging for follow-up of these patients revealed various nonvascular complications such as aseptic meningitis, hydrocephalus, and perianeurysmal brain edema. We present 7 patients from 5 different institutions that developed MR imaging-enhancing brain lesions after endovascular therapy of aneurysms, detected after a median time of 63 days. The number of lesions ranged from 4-46 (median of 10.5), sized 2-20 mm, and were mostly in the same vascular territory used for access. Three patients presented with symptoms attributable to these lesions. After a median follow-up of 21.5 months, the number of lesions increased in 2, was stable in 1, decreased in 3, and disappeared in 1. The imaging and clinical characteristics suggested a foreign body reaction. We could find no correlation to a specific device, but a possible source may be the generic hydrophilic coating.
© 2014 by American Journal of Neuroradiology.
Figures

References
-
- Molyneux AJ, Kerr RS, Birks J, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): long-term follow-up. Lancet Neurol 2009;8:427–33 - PMC - PubMed
-
- Spetzler RF, McDougall CG, Albuquerque FC, et al. The Barrow ruptured aneurysm trial: 3-year results. J Neurosurg 2013;119:146–57 - PubMed
-
- Pierot L, Wakhloo AK. Endovascular treatment of intracranial aneurysms: current status. Stroke 2013;44:2046–54 - PubMed
-
- Fanning NF, Willinsky RA, ter Brugge KG. Wall enhancement, edema, and hydrocephalus after endovascular coil occlusion of intradural cerebral aneurysms. J Neurosurg 2008;108:1074–86 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical