

Predictors of functional dependence despite successful revascularization in large-vessel occlusion strokes
- PMID: 24876082
- PMCID: PMC4160889
- DOI: 10.1161/STROKEAHA.114.005603
Predictors of functional dependence despite successful revascularization in large-vessel occlusion strokes
Abstract
Background and purpose: High revascularization rates in large-vessel occlusion strokes treated by mechanical thrombectomy are not always associated with good clinical outcomes. We evaluated predictors of functional dependence despite successful revascularization among patients with acute ischemic stroke treated with thrombectomy.
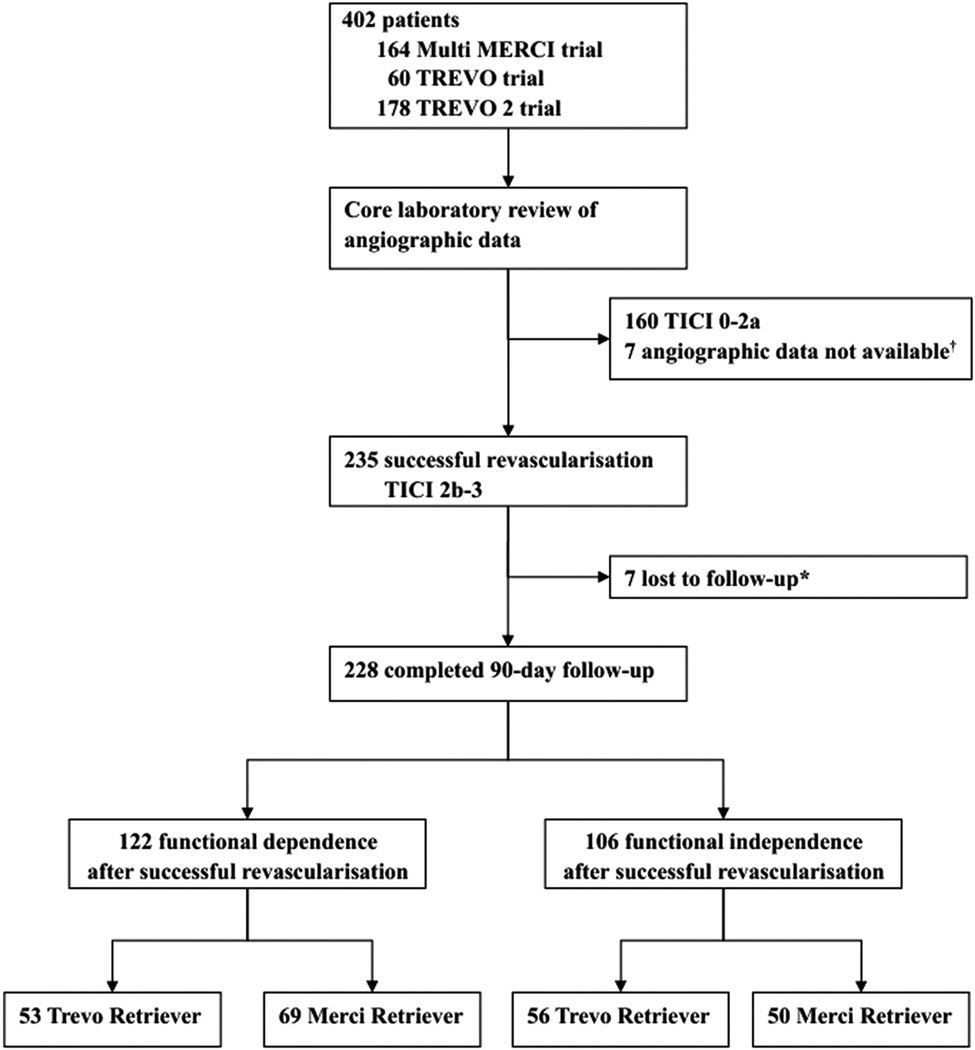
Methods: We analyzed the pooled data from the Multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI), Thrombectomy Revascularization of Large Vessel Occlusions in Acute Ischemic Stroke (TREVO), and TREVO 2 trials. Successful revascularization was defined as thrombolysis in cerebral infarction score 2b or 3. Functional dependence was defined as a score of 3 to 6 on the modified Rankin Scale at 3 months. We assessed relationship of demographic, clinical, angiographic characteristics, and hemorrhage with functional dependence despite successful revascularization.
Results: Two hundred and twenty-eight patients with successful revascularization had clinical outcome follow-up. The rates of functional dependence with endovascular success were 48.6% for Trevo thrombectomy and 58.0% for Merci thrombectomy. Age (odds ratio, 1.04; 95% confidence interval, 1.02-1.06 per 1-year increase), National Institutes of Health Stroke Scale score (odds ratio, 1.08; 95% confidence interval, 1.02-1.15 per 1-point increase), and symptom onset to endovascular treatment time (odds ratio, 1.11; 95% confidence interval, 1.01-1.22 per 30-minute delay) were predictors of functional dependence despite successful revascularization. Symptom onset to reperfusion time beyond 5 hours was associated with functional dependence. All subjects with symptomatic intracranial hemorrhage had functional dependence.
Conclusions: One half of patients with successful mechanical thrombectomy do not have good outcomes. Age, severe neurological deficits, and delayed endovascular treatment were associated with functional dependence despite successful revascularization. Our data support efforts to minimize delays to endovascular therapy in patients with acute ischemic stroke to improve outcomes.
Clinical trial registration url: http://www.clinicaltrials.gov. Unique identifier: NCT00318071, NCT01088672, and NCT01270867.
Keywords: stroke.
© 2014 American Heart Association, Inc.
Figures
References
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Alexandrov AV, Molina CA, Grotta JC, Garami Z, Ford SR, Alvarez-Sabin J, et al. CLOTBUST Investigators. Ultrasound-enhanced systemic thrombolysis for acute ischemic stroke. N Engl J Med. 2004;351:2170–2178. - PubMed
-
- Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA. 1999;282:2003–2011. - PubMed
-
- Smith WS, Sung G, Saver J, Budzik R, Duckwiler G, Liebeskind DS, et al. Multi MERCI Investigators. Mechanical thrombectomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke. 2008;39:1205–1212. - PubMed
-
- Goyal M, Menon BK, Coutts SB, Hill MD, Demchuk AM. Penumbra Pivotal Stroke Trial Investigators, Calgary Stroke Program, and the Seaman MR Research Center. Effect of baseline CT scan appearance and time to recanalization on clinical outcomes in endovascular thrombectomy of acute ischemic strokes. Stroke. 2011;42:93–97. - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
