

Pretreatment blood-brain barrier damage and post-treatment intracranial hemorrhage in patients receiving intravenous tissue-type plasminogen activator
- PMID: 24876245
- PMCID: PMC4120660
- DOI: 10.1161/STROKEAHA.114.005249
Pretreatment blood-brain barrier damage and post-treatment intracranial hemorrhage in patients receiving intravenous tissue-type plasminogen activator
Abstract
Background and purpose: Early blood-brain barrier damage after acute ischemic stroke has previously been qualitatively linked to subsequent intracranial hemorrhage (ICH). In this quantitative study, it was investigated whether the amount of blood-brain barrier damage evident on pre-tissue-type plasminogen activator MRI scans was related to the degree of post-tissue-type plasminogen activator ICH in patients with acute ischemic stroke.
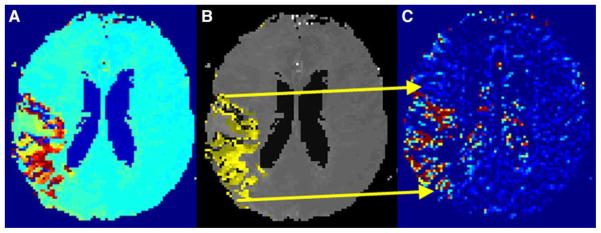
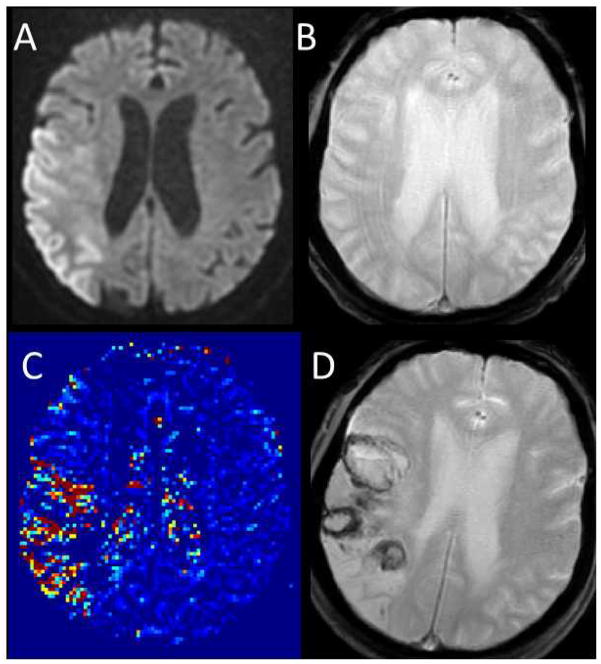
Methods: Analysis was performed on a database of patients with acute ischemic stroke provided by the Stroke Imaging Repository (STIR) and Virtual International Stroke Trials Archive (VISTA) Imaging Investigators. Patients with perfusion-weighted imaging lesions>10 mL and negative gradient-recalled echo imaging before intravenous tissue-type plasminogen activator were included. Postprocessing of the perfusion-weighted imaging source images was performed to estimate changes in blood-brain barrier permeability within the perfusion deficit relative to the unaffected hemisphere. Follow-up gradient-recalled echo images were reviewed for evidence of ICH and divided into 3 groups according to European Cooperative Acute Stroke Study (ECASS) criteria: no hemorrhage, hemorrhagic infarction, and parenchymal hematoma.
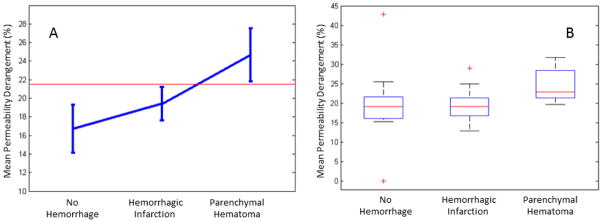
Results: Seventy-five patients from the database met the inclusion criteria, 28 of whom experienced ICH, of which 19 were classified as hemorrhagic infarction and 9 were classified as parenchymal hematoma. The mean permeability (±SDs), expressed as an index of contrast leakage, was 17.0±8.8% in the no hemorrhage group, 19.4±4.0% in the hemorrhagic infarction group, and 24.6±4.5% in the parenchymal hematoma group. Permeability was significantly correlated with ICH grade in univariate (P=0.007) and multivariate (P=0.008) linear regression modeling.
Conclusions: A perfusion-weighted imaging-derived index of blood-brain barrier damage measured before intravenous tissue-type plasminogen activator is given is associated with the severity of ICH after treatment in patients with acute ischemic stroke.
Keywords: blood–brain barrier; magnetic resonance imaging; stroke.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Peter B. Barker has served as a consultant to Olea Medical.
Figures
References
-
- The national institute of neurological disorders and stroke rt-pa stroke study group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von KR, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The european cooperative acute stroke study (ecass) JAMA. 1995;274:1017–1025. - PubMed
-
- The ninds t-pa stroke study group. Intracerebral hemorrhage after intravenous t-pa therapy for ischemic stroke. Stroke. 1997;28:2109–2118. - PubMed
-
- Hjort N, Wu O, Ashkanian M, Solling C, Mouridsen K, Christensen S, et al. Mri detection of early blood-brain barrier disruption: Parenchymal enhancement predicts focal hemorrhagic transformation after thrombolysis. Stroke. 2008;39:1025–1028. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
