

Drivers of costs associated with reperfusion therapy in acute stroke: the Interventional Management of Stroke III Trial
- PMID: 24876261
- PMCID: PMC4128893
- DOI: 10.1161/STROKEAHA.113.003874
Drivers of costs associated with reperfusion therapy in acute stroke: the Interventional Management of Stroke III Trial
Abstract
Background and purpose: The Interventional Management of Stroke (IMS) III study tested the effect of intravenous tissue-type plasminogen activator (tPA) alone when compared with intravenous tPA followed by endovascular therapy and collected cost data to assess the economic implications of the 2 therapies. This report describes the factors affecting the costs of the initial hospitalization for acute stroke subjects from the United States.
Methods: Prospective cost analysis of the US subjects was treated with intravenous tPA alone or with intravenous tPA followed by endovascular therapy in the IMS III trial. Results were compared with expected Medicare payments.
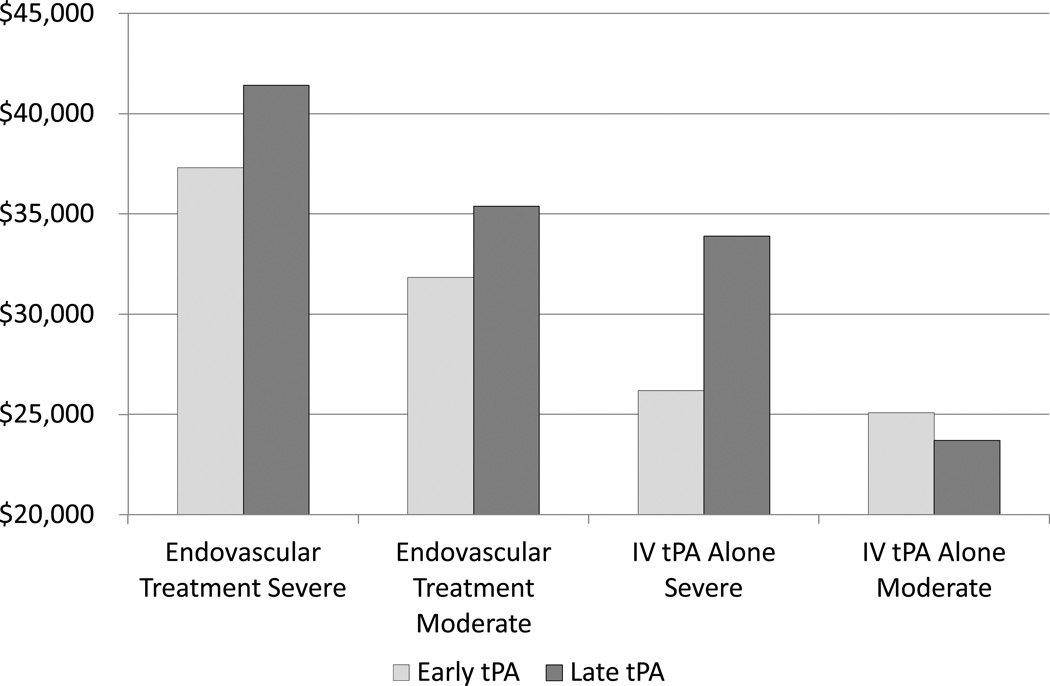
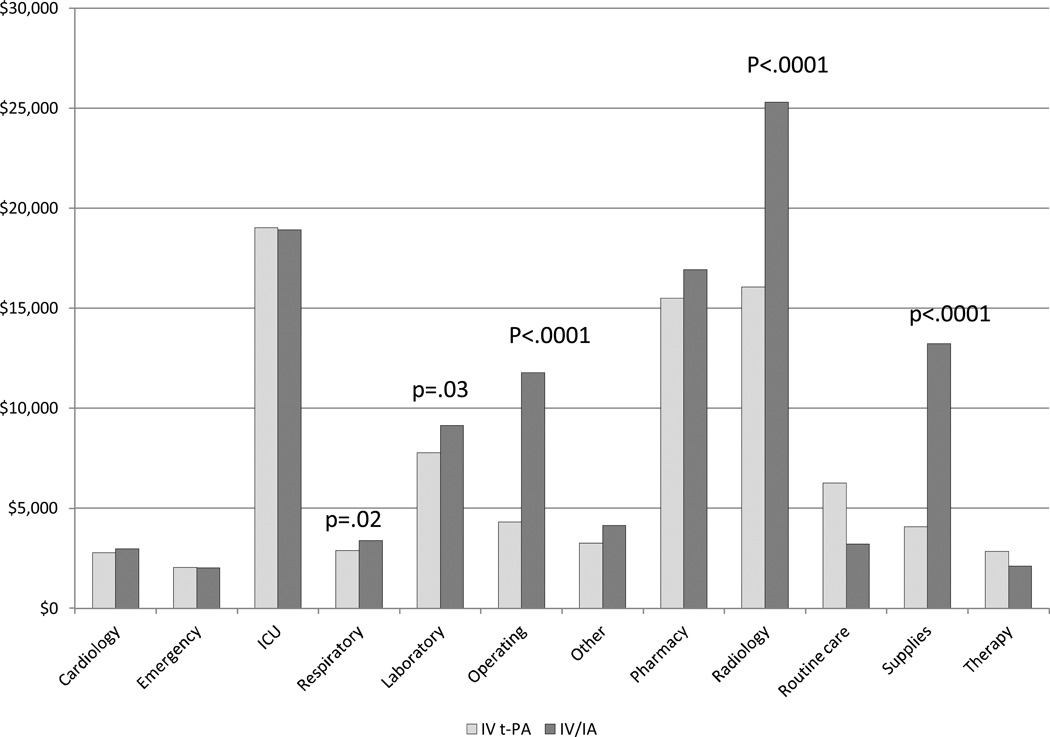
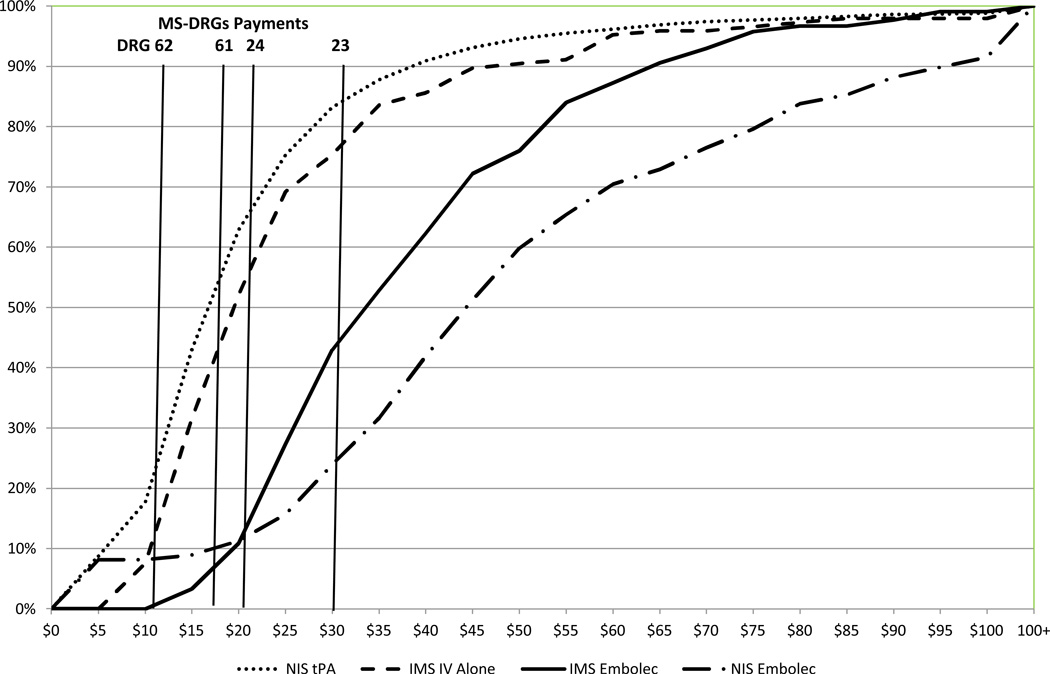
Results: The adjusted cost of a stroke admission in the study was $35 130 for subjects treated with endovascular therapy after intravenous tPA treatment and $25 630 for subjects treated with intravenous tPA alone (P<0.0001). Significant factors related to costs included treatment group, baseline National Institutes of Health Stroke Scale, time from stroke onset to intravenous tPA, age, stroke location, and comorbid diabetes mellitus. The mean cost for subjects who had routine use of general anesthesia as part of endovascular therapy was $46 444 when compared with $30 350 for those who did not have general anesthesia. The costs of embolectomy for IMS III subjects and patients from the National Inpatient Sample cohort exceeded the Medicare diagnosis-related group payment in ≥75% of patients.
Conclusions: Minimizing the time to start of intravenous tPA and decreasing the use of routine general anesthesia may improve the cost-effectiveness of medical and endovascular therapy for acute stroke.
Clinical trial registration url: http://www.clinicaltrials.gov. Unique identifier: NCT00359424.
Keywords: brain ischemic; costs and cost analysis; hospitals; reperfusion; stroke.
© 2014 American Heart Association, Inc.
Figures
References
-
- Brinjikji W, Rabinstein AA, Cloft HJ. Hospitalization costs for acute ischemic stroke patients treated with intravenous thrombolysis in the United States are substantially higher tha Medicare payments. Stroke. 2012;43:1131–1133. - PubMed
-
- Fonarow GC, Pan W, Saver JL, Smith EE, Reeves MJ, Broderick JP, et al. Comparison of 30-Day Mortality Models for Profiling Hospital Performance in Acute Ischemic Stroke With vs Without Adjustment for Stroke Severity. JAMA. 2012;308:257–264. - PubMed
-
- Guzauskas GF, Boudreau DM, Villa KF, Levine SR, Veenstra DL. The Cost-Effectiveness of Primary Stroke Centers for Acute Stroke Care. Stroke. 2012;43:1617–1623. - PubMed
-
- Fagan SC, Morgenstern LB, Petitta A, Ward RE, Tilley BC, Marler JR, et al. Cost-effectiveness of tissue plasminogen activator for acute ischemic stroke. NINDS rt-PA Stroke Study Group. Neurology. 1998;50:883–890. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
