

Component separation in abdominal trauma
- PMID: 24876334
- PMCID: PMC3913436
- DOI: 10.1093/jscr/rjt133
Component separation in abdominal trauma
Abstract
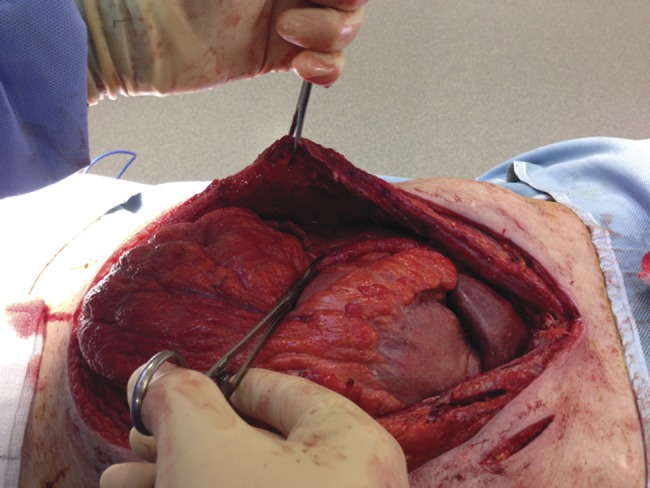
Component separation is established for complex hernia repairs. This case presents early component separation and release of the anterior and posterior sheath to facilitate closure of the abdominal wall following emergency laparotomy, reinforcing the repair with a biological mesh. On Day 11 following an emergency laparotomy for penetrating trauma, this patient underwent component separation and release of the anterior and posterior sheath. An intra-abdominal biological mesh was secured, and the fascia and skin closed successfully. Primary abdominal closure can be achieved in patients with penetrating abdominal trauma with the use of component separation and insertion of intra-abdominal biological mesh, where standard closure is not possible.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author 2014.
Figures





References
-
- Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990;86:519–26. - PubMed
-
- de Vries Reilingh TS, van Goor H, Rosman C, Bemelmans MH, de Jong D, van Nieuwenhoven EJ, et al. “Components separation technique” for the repair of large abdominal wall hernias. J Am Coll Surg. 2003;196:32–7. - PubMed
-
- Clarke JM. Incisional hernia repair by fascial component separation: results in 128 cases and evolution of technique. Am J Surg. 2010;200:2–8. - PubMed
-
- Hood K, Millikan K, Pittman T, Zelhart M, Secemsky B, Rajan M, et al. Abdominal wall reconstruction: a case series of ventral hernia repair using the component separation technique with biologic mesh. Am J Surg. 2013;205:322–7. discussion 327–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
