

Design and implementation of a web-based reporting and benchmarking center for inpatient glucometrics
- PMID: 24876426
- PMCID: PMC4764218
- DOI: 10.1177/1932296814532237
Design and implementation of a web-based reporting and benchmarking center for inpatient glucometrics
Abstract
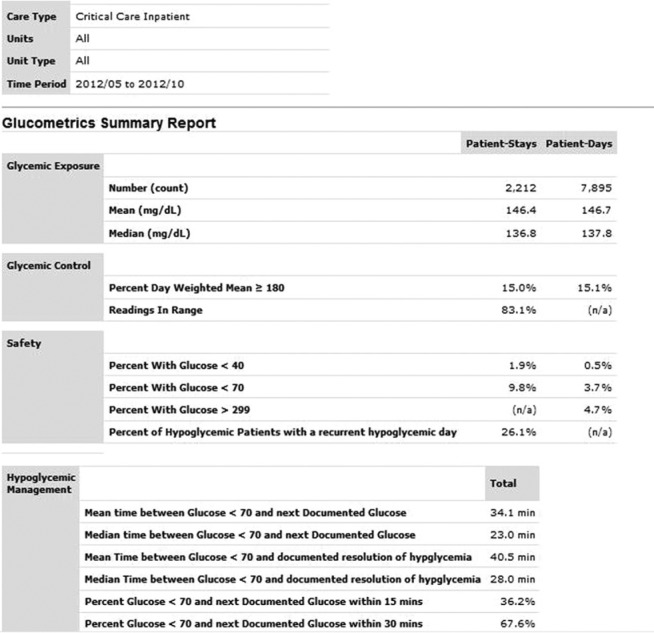
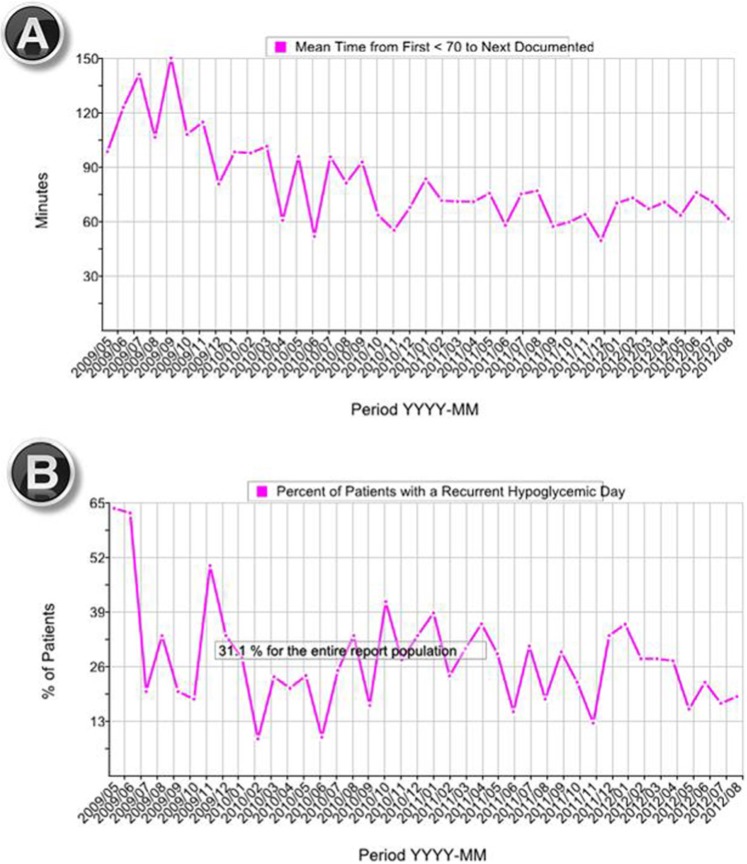
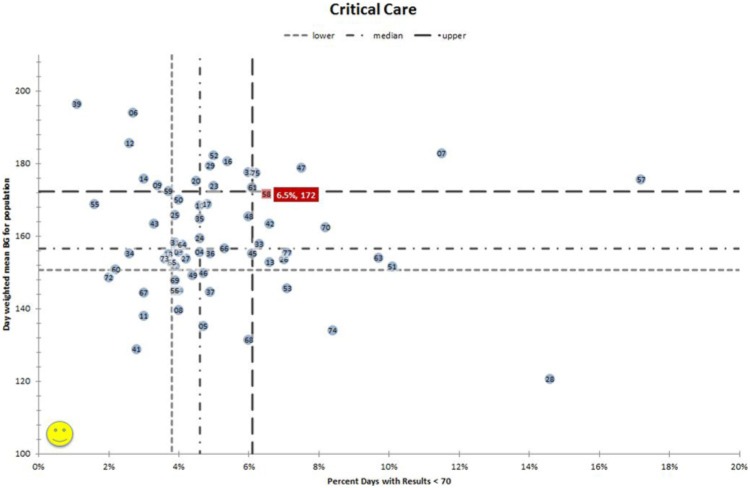
Insulin is a top source of adverse drug events in the hospital, and glycemic control is a focus of improvement efforts across the country. Yet, the majority of hospitals have no data to gauge their performance on glycemic control, hypoglycemia rates, or hypoglycemic management. Current tools to outsource glucometrics reports are limited in availability or function. Society of Hospital Medicine (SHM) faculty designed and implemented a web-based data and reporting center that calculates glucometrics on blood glucose data files securely uploaded by users. Unit labels, care type (critical care, non-critical care), and unit type (eg, medical, surgical, mixed, pediatrics) are defined on upload allowing for robust, flexible reporting. Reports for any date range, care type, unit type, or any combination of units are available on demand for review or downloading into a variety of file formats. Four reports with supporting graphics depict glycemic control, hypoglycemia, and hypoglycemia management by patient day or patient stay. Benchmarking and performance ranking reports are generated periodically for all hospitals in the database. In all, 76 hospitals have uploaded at least 12 months of data for non-critical care areas and 67 sites have uploaded critical care data. Critical care benchmarking reveals wide variability in performance. Some hospitals achieve top quartile performance in both glycemic control and hypoglycemia parameters. This new web-based glucometrics data and reporting tool allows hospitals to track their performance with a flexible reporting system, and provides them with external benchmarking. Tools like this help to establish standardized glucometrics and performance standards.
Keywords: benchmarking; blood glucose monitoring; diabetes; glycemic control; hospital; hyperglycemia; hypoglycemia; quality improvement.
© 2014 Diabetes Technology Society.
Conflict of interest statement
Figures


References
-
- Centers for Disease Control and Prevention. Hospitalizations for Diabetes and Any-Listed Diagnosis. Available at: http://www.cdc.gov/diabetes/statistics/dmany/index.htm. Accessed December 2012.
-
- National Quality Forum. Safe Practices for Better Healthcare–2010 Update: A Consensus Report. Safe Practice 32: Glycemic Control. Washington, DC: NQF; 2010.
-
- Umpierrez GE, Hellman R, Korytkowski MT, et al. Management of hyperglycemia in hospitalized patients in the non-critical care setting: an endocrine society clinical practice guideline. J Clin Endocrinol Metabol. 2012;97(1):16-38. - PubMed
-
- Hellman R. A systems approach to reducing errors in insulin therapy in the inpatient setting. Endocr Pract. 2006;12(S3):49-55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
