

Prognostic factors for hepatocellular carcinoma recurrence
- PMID: 24876717
- PMCID: PMC4033434
- DOI: 10.3748/wjg.v20.i20.5935
Prognostic factors for hepatocellular carcinoma recurrence
Abstract
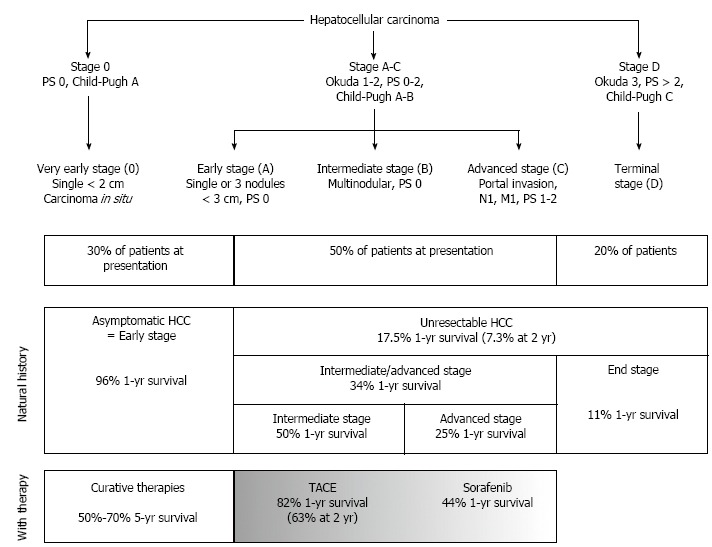
The recurrence of hepatocellular carcinoma, the sixth most common neoplasm and the third leading cause of cancer-related mortality worldwide, represents an important clinical problem, since it may occur after both surgical and medical treatment. The recurrence rate involves 2 phases: an early phase and a late phase. The early phase usually occurs within 2 years after resection; it is mainly related to local invasion and intrahepatic metastases and, therefore, to the intrinsic biology of the tumor. On the other hand, the late phase occurs more than 2 years after surgery and is mainly related to de novo tumor formation as a consequence of the carcinogenic cirrhotic environment. Since recent studies have reported that early and late recurrences may have different risk factors, it is clinically important to recognize these factors in the individual patient as soon as possible. The aim of this review was, therefore, to identify predicting factors for the recurrence of hepatocellular carcinoma, by means of invasive and non-invasive methods, according to the different therapeutic strategies available. In particular the role of emerging techniques (e.g., transient elastography) and biological features of hepatocellular carcinoma in predicting recurrence have been discussed. In particular, invasive methods were differentiated from non-invasive ones for research purposes, taking into consideration the emerging role of the genetic signature of hepatocellular carcinoma in order to better allocate treatment strategies and surveillance follow-up in patients with this type of tumor.
Keywords: Hepatic resection; Hepatocellular carcinoma; Liver biopsy; Liver stiffness measurement; Orthotopic liver transplant; Percutaneous ethanol injection; Percutaneous radiofrequency ablation; Transarterial chemoembolization.
Figures
References
-
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245–1255. - PubMed
-
- El-Serag HB. Hepatocellular carcinoma. N Engl J Med. 2011;365:1118–1127. - PubMed
-
- European Association For The Study Of The Liver; European Organisation For Research And Treatment Of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56:908–943. - PubMed
-
- Bolondi L, Cillo U, Colombo M, Craxì A, Farinati F, Giannini EG, Golfieri R, Levrero M, Pinna AD, Piscaglia F, et al. Position paper of the Italian Association for the Study of the Liver (AISF): the multidisciplinary clinical approach to hepatocellular carcinoma. Dig Liver Dis. 2013;45:712–723. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
