

Post-operative imaging in liver transplantation: state-of-the-art and future perspectives
- PMID: 24876739
- PMCID: PMC4033456
- DOI: 10.3748/wjg.v20.i20.6180
Post-operative imaging in liver transplantation: state-of-the-art and future perspectives
Abstract
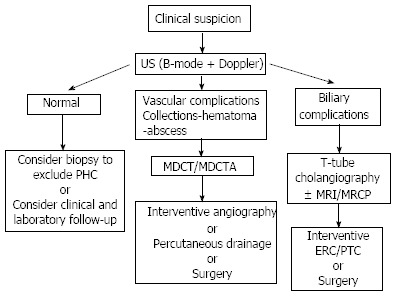
Orthotopic liver transplantation (OLT) represents a major treatment for end-stage chronic liver disease, as well as selected cases of hepatocellular carcinoma and acute liver failure. The ever-increasing development of imaging modalities significantly contributed, over the last decades, to the management of recipients both in the pre-operative and post-operative period, thus impacting on graft and patients survival. When properly used, imaging modalities such as ultrasound, multidetector computed tomography, magnetic resonance imaging (MRI) and procedures of direct cholangiography are capable to provide rapid and reliable recognition and treatment of vascular and biliary complications occurring after OLT. Less defined is the role for imaging in assessing primary graft dysfunction (including rejection) or chronic allograft disease after OLT, e.g., hepatitis C virus (HCV) recurrence. This paper: (1) describes specific characteristic of the above imaging modalities and the rationale for their use in clinical practice; (2) illustrates main imaging findings related to post-OLT complications in adult patients; and (3) reviews future perspectives emerging in the surveillance of recipients with HCV recurrence, with special emphasis on MRI.
Keywords: Computed tomography; Endoscopic retrograde cholangiography; Human C virus recurrence; Magnetic resonance imaging; Orthotopic liver transplantation; Orthotopic liver transplantation complications; Percutaneous transhepatic cholangiography; T-tube cholangiography; Ultrasound.
Figures

References
-
- Itri JN, Heller MT, Tublin ME. Hepatic transplantation: postoperative complications. Abdom Imaging. 2013;38:1300–1333. - PubMed
-
- Boraschi P, Donati F. Complications of orthotopic liver transplantation: imaging findings. Abdom Imaging. 2004;29:189–202. - PubMed
-
- García-Criado A, Gilabert R, Bargalló X, Brú C. Radiology in liver transplantation. Semin Ultrasound CT MR. 2002;23:114–129. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
