

Task-based strategy for optimized contrast enhanced breast imaging: analysis of six imaging techniques for mammography and tomosynthesis
- PMID: 24877819
- PMCID: PMC4032404
- DOI: 10.1118/1.4873317
Task-based strategy for optimized contrast enhanced breast imaging: analysis of six imaging techniques for mammography and tomosynthesis
Abstract
Purpose: The use of contrast agents in breast imaging has the capability of enhancing nodule detectability and providing physiological information. Accordingly, there has been a growing trend toward using iodine as a contrast medium in digital mammography (DM) and digital breast tomosynthesis (DBT). Widespread use raises concerns about the best way to use iodine in DM and DBT, and thus a comparison is necessary to evaluate typical iodine-enhanced imaging methods. This study used a task-based observer model to determine the optimal imaging approach by analyzing six imaging paradigms in terms of their ability to resolve iodine at a given dose: unsubtracted mammography and tomosynthesis, temporal subtraction mammography and tomosynthesis, and dual energy subtraction mammography and tomosynthesis.
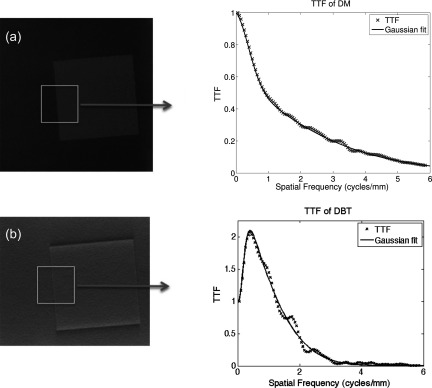
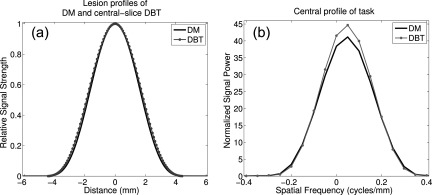
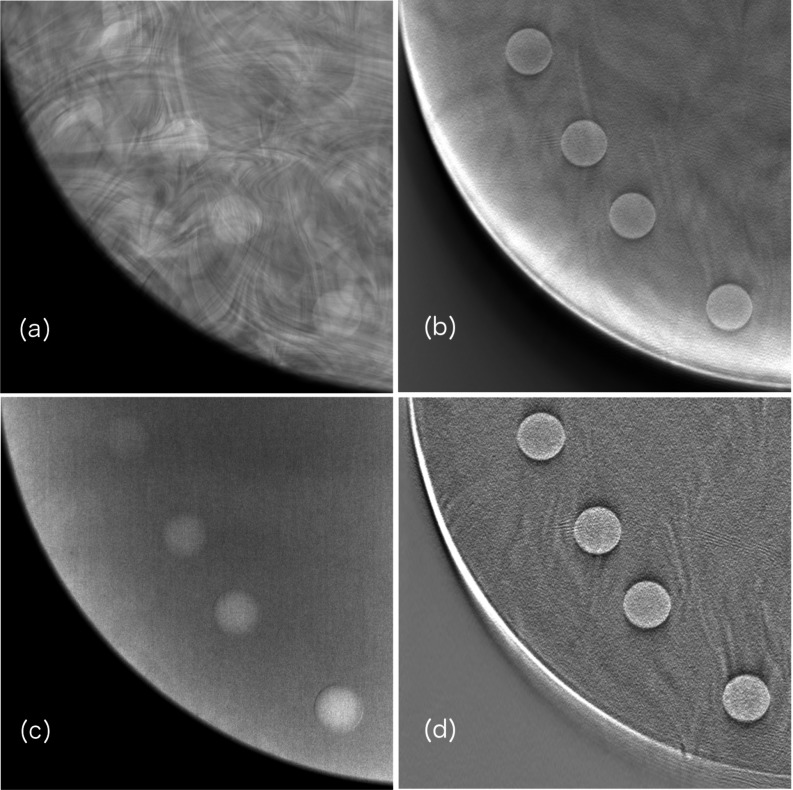
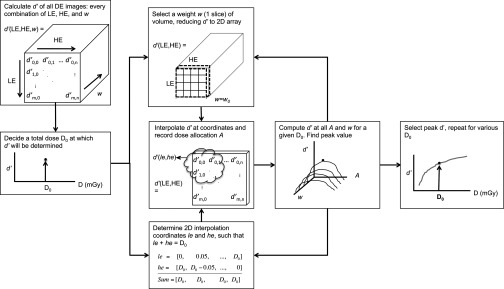
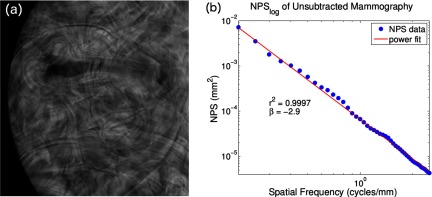
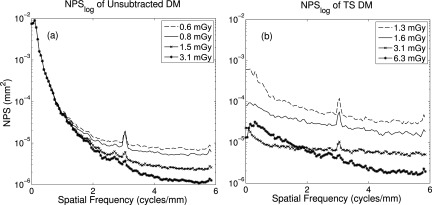
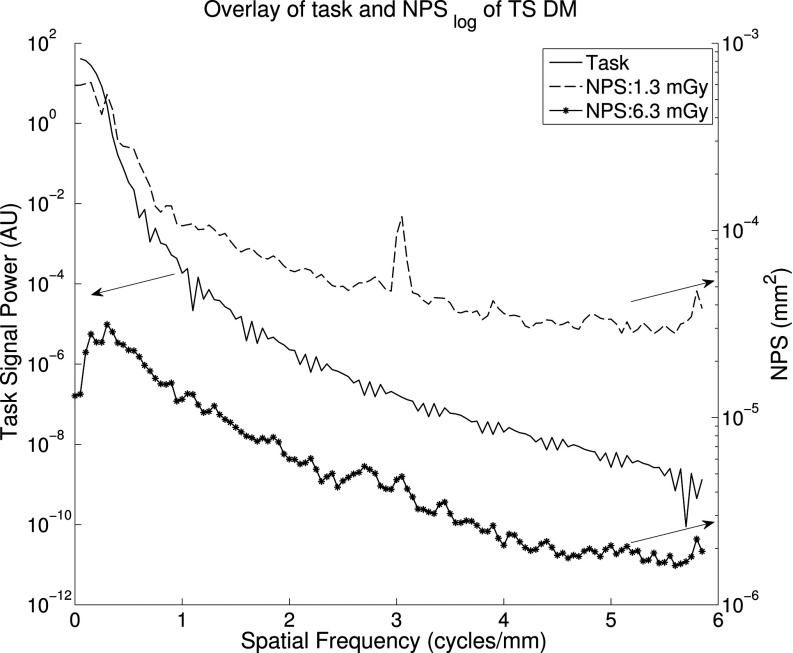
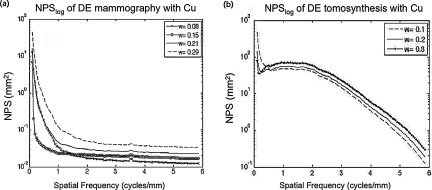
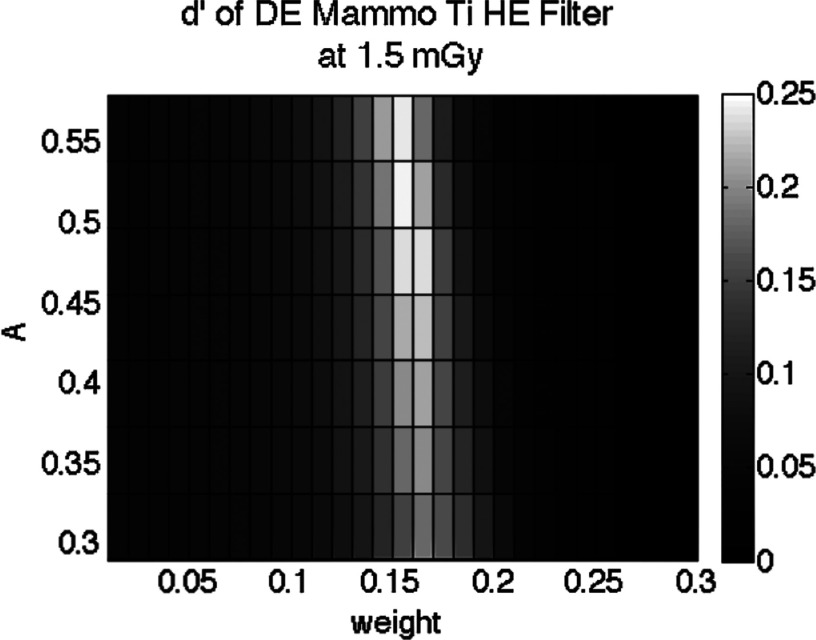
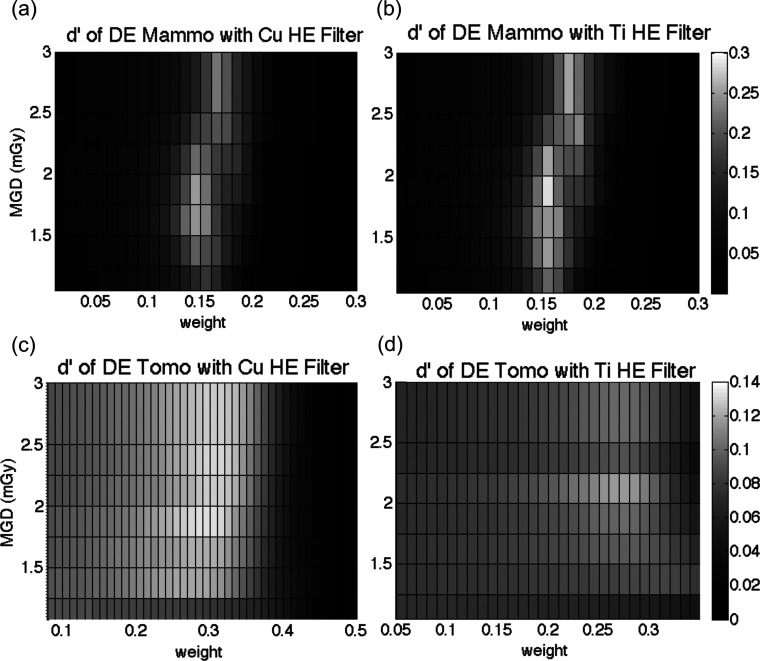
Methods: Imaging performance was characterized using a detectability index d', derived from the system task transfer function (TTF), an imaging task, iodine signal difference, and the noise power spectrum (NPS). The task modeled a 10 mm diameter lesion containing iodine concentrations between 2.1 mg/cc and 8.6 mg/cc. TTF was obtained using an edge phantom, and the NPS was measured over several exposure levels, energies, and target-filter combinations. Using a structured CIRS phantom, d' was generated as a function of dose and iodine concentration.
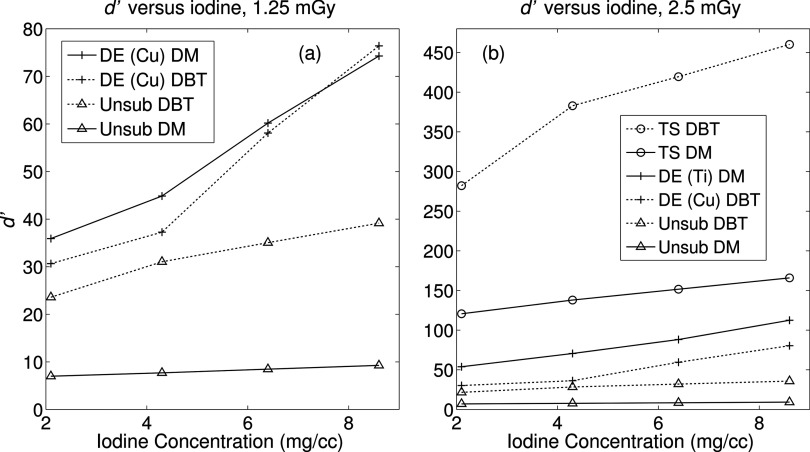
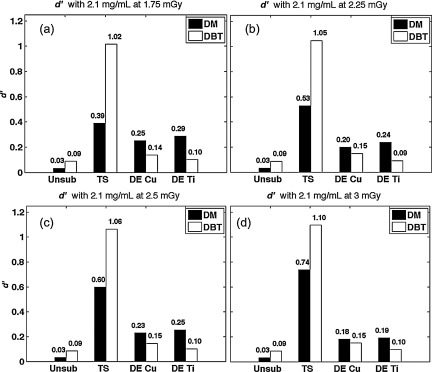
Results: For all iodine concentrations and dose, temporal subtraction techniques for mammography and tomosynthesis yielded the highest d', while dual energy techniques for both modalities demonstrated the next best performance. Unsubtracted imaging resulted in the lowest d' values for both modalities, with unsubtracted mammography performing the worst out of all six paradigms.
Conclusions: At any dose, temporal subtraction imaging provides the greatest detectability, with temporally subtracted DBT performing the highest. The authors attribute the successful performance to excellent cancellation of inplane structures and improved signal difference in the lesion.
Figures

Similar articles
-
Optimization of contrast-enhanced breast imaging: Analysis using a cascaded linear system model.Med Phys. 2017 Jan;44(1):43-56. doi: 10.1002/mp.12004. Epub 2017 Jan 3. Med Phys. 2017. PMID: 28044312
-
Phantom study to evaluate contrast-medium-enhanced digital subtraction mammography with a full-field indirect-detection system.Med Phys. 2010 Feb;37(2):577-89. doi: 10.1118/1.3276733. Med Phys. 2010. PMID: 20229866
-
The effect of amorphous selenium detector thickness on dual-energy digital breast imaging.Med Phys. 2014 Nov;41(11):111904. doi: 10.1118/1.4897244. Med Phys. 2014. PMID: 25370637 Free PMC article.
-
Evaluation of the minimum iodine concentration for contrast-enhanced subtraction mammography.Phys Med Biol. 2006 Sep 7;51(17):4233-51. doi: 10.1088/0031-9155/51/17/008. Epub 2006 Aug 8. Phys Med Biol. 2006. PMID: 16912379
-
Task-based detectability in anatomical background in digital mammography, digital breast tomosynthesis and synthetic mammography.Phys Med Biol. 2024 Jan 12;69(2). doi: 10.1088/1361-6560/ad1766. Phys Med Biol. 2024. PMID: 38214048
Cited by
-
Virtual clinical trials in medical imaging: a review.J Med Imaging (Bellingham). 2020 Jul;7(4):042805. doi: 10.1117/1.JMI.7.4.042805. Epub 2020 Apr 11. J Med Imaging (Bellingham). 2020. PMID: 32313817 Free PMC article. Review.
-
Physics considerations in MV-CBCT multi-layer imager design.Phys Med Biol. 2018 Jun 20;63(12):125016. doi: 10.1088/1361-6560/aac8c6. Phys Med Biol. 2018. PMID: 29846180 Free PMC article.
-
Impact of Tomosynthesis Acquisition on 3D Segmentations of Breast Outline and Adipose/Dense Tissue with AI: A Simulation-Based Study.Tomography. 2023 Jul 3;9(4):1303-1314. doi: 10.3390/tomography9040103. Tomography. 2023. PMID: 37489471 Free PMC article.
-
Frequency-dependent signal and noise in spectroscopic x-ray imaging.Med Phys. 2020 Jul;47(7):2881-2901. doi: 10.1002/mp.14160. Epub 2020 Apr 22. Med Phys. 2020. PMID: 32239517 Free PMC article.
-
Phantom-based study exploring the effects of different scatter correction approaches on the reconstructed images generated by contrast-enhanced stationary digital breast tomosynthesis.J Med Imaging (Bellingham). 2018 Jan;5(1):013502. doi: 10.1117/1.JMI.5.1.013502. Epub 2018 Feb 1. J Med Imaging (Bellingham). 2018. PMID: 29430472 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
