

Quality of care and racial disparities in medicare among potential ACOs
- PMID: 24879050
- PMCID: PMC4139518
- DOI: 10.1007/s11606-014-2900-3
Quality of care and racial disparities in medicare among potential ACOs
Abstract
Background: The Medicare Accountable Care Organization (ACO) programs encourage integration of providers into large groups and reward provider groups for improving quality, but not explicitly for reducing health care disparities. Larger group size and better overall quality may or may not be associated with smaller disparities.
Objective: To examine differences in patient characteristics between provider groups sufficiently large to participate in ACO programs and smaller groups; the association between group size and racial disparities in quality; and the association between quality and disparities among larger groups.
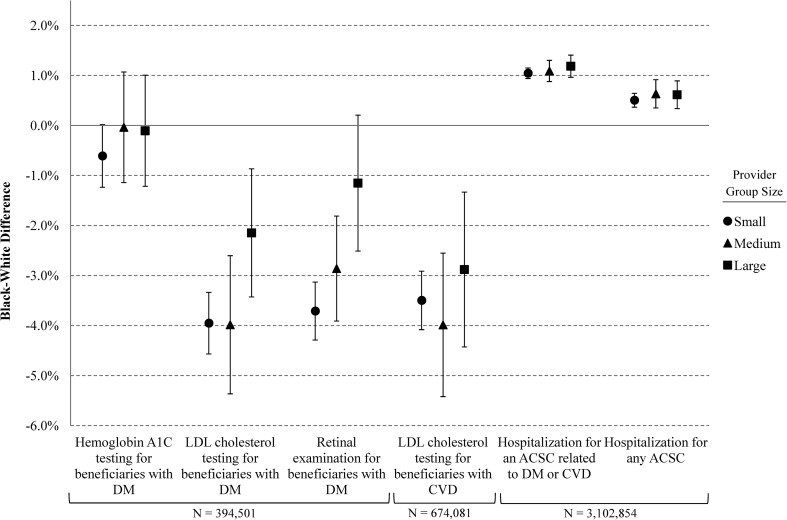
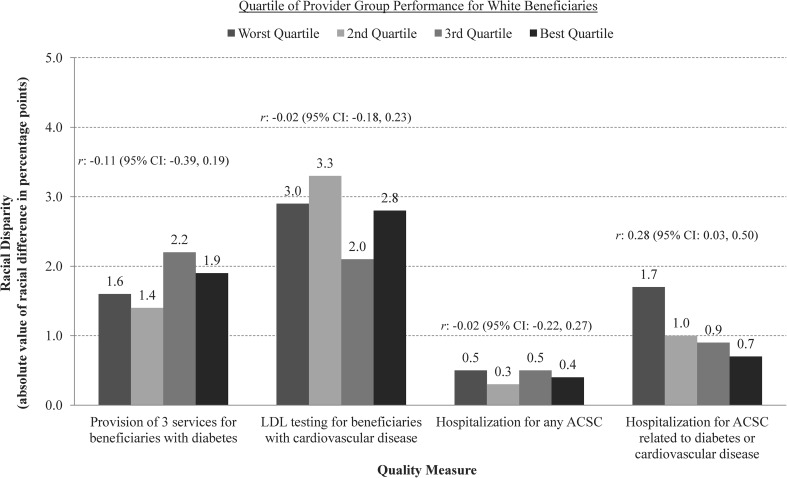
Design and participants: Using 2009 Medicare claims for 3.1 million beneficiaries with cardiovascular disease or diabetes and linked data on provider groups, we compared racial differences in quality by provider group size, adjusting for patient characteristics. Among larger groups, we used multilevel models to estimate correlations between group performance on quality measures for white beneficiaries and black-white disparities within groups.
Main measures: Four process measures of quality, hospitalization for ambulatory care-sensitive conditions (ACSCs) related to cardiovascular disease or diabetes, and hospitalization for any ACSC.
Key results: Beneficiaries served by larger groups were more likely to be white and live in areas with less poverty and more education. Larger group size was associated with smaller disparities in low-density lipoprotein (LDL) cholesterol testing and retinal exams, but not in other process measures or hospitalization for ACSCs. Among larger groups, better quality for white beneficiaries in one measure (hospitalization for ACSCs related to cardiovascular disease or diabetes) was correlated with smaller racial disparities (r = 0.28; P = 0.02), but quality was not correlated with disparities in other measures.
Conclusions: Larger provider group size and better performance on quality measures were not consistently associated with smaller racial disparities in care for Medicare beneficiaries with cardiovascular disease or diabetes. ACO incentives rewarding better quality for minority groups and payment arrangements supporting ACO development in disadvantaged communities may be required for ACOs to promote greater equity in care.
Figures


Comment in
-
Capsule commentary on Anderson et al., quality of care and racial disparities in medicare among potential ACOs.J Gen Intern Med. 2014 Sep;29(9):1273. doi: 10.1007/s11606-014-2934-6. J Gen Intern Med. 2014. PMID: 25002160 Free PMC article. No abstract available.
Similar articles
-
Capsule commentary on Anderson et al., quality of care and racial disparities in medicare among potential ACOs.J Gen Intern Med. 2014 Sep;29(9):1273. doi: 10.1007/s11606-014-2934-6. J Gen Intern Med. 2014. PMID: 25002160 Free PMC article. No abstract available.
-
Association Between Organizational Quality and Out-of-Network Primary Care Among Accountable Care Organizations That Care for High vs Low Proportions of Patients of Racial and Ethnic Minority Groups.JAMA Health Forum. 2022 Apr 15;3(4):e220575. doi: 10.1001/jamahealthforum.2022.0575. eCollection 2022 Apr. JAMA Health Forum. 2022. PMID: 35977323 Free PMC article.
-
Trends in the quality of care and racial disparities in Medicare managed care.N Engl J Med. 2005 Aug 18;353(7):692-700. doi: 10.1056/NEJMsa051207. N Engl J Med. 2005. PMID: 16107622
-
Racial disparities in outcomes after cardiac surgery: the role of hospital quality.Curr Cardiol Rep. 2015 May;17(5):29. doi: 10.1007/s11886-015-0587-7. Curr Cardiol Rep. 2015. PMID: 25894800 Free PMC article. Review.
-
Building an Infrastructure to Address Racial Disparities in Treatment and Outcomes in Children with Type 1 Diabetes.Endocrinol Metab Clin North Am. 2025 Jun;54(2):217-224. doi: 10.1016/j.ecl.2025.03.004. Epub 2025 Apr 11. Endocrinol Metab Clin North Am. 2025. PMID: 40348563 Review.
Cited by
-
Patient and provider-level factors associated with changes in utilization of treatments in response to evidence on ineffectiveness or harm.Int J Health Econ Manag. 2020 Sep;20(3):299-317. doi: 10.1007/s10754-020-09282-2. Epub 2020 Apr 30. Int J Health Econ Manag. 2020. PMID: 32350680 Free PMC article.
-
Association of Physician Group Participation in Accountable Care Organizations With Patient Social and Clinical Characteristics.JAMA Netw Open. 2019 Jan 4;2(1):e187220. doi: 10.1001/jamanetworkopen.2018.7220. JAMA Netw Open. 2019. PMID: 30657535 Free PMC article.
-
Association of Medicare Advantage Star Ratings With Racial, Ethnic, and Socioeconomic Disparities in Quality of Care.JAMA Health Forum. 2021 Jun 11;2(6):e210793. doi: 10.1001/jamahealthforum.2021.0793. eCollection 2021 Jun. JAMA Health Forum. 2021. PMID: 35977175 Free PMC article.
-
Racial and Ethnic Disparities in Preventive and Chronic Disease Care in Medicare Advantage vs. Traditional Medicare.J Gen Intern Med. 2025 Aug 11. doi: 10.1007/s11606-025-09793-z. Online ahead of print. J Gen Intern Med. 2025. PMID: 40790002
-
Advancing Health Services Research to Eliminate Health Care Disparities.Am J Public Health. 2019 Jan;109(S1):S64-S69. doi: 10.2105/AJPH.2018.304922. Am J Public Health. 2019. PMID: 30699021 Free PMC article.
References
-
- Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations; Final Rule, 42 CFR Part 425. (2011). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
