

Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people
- PMID: 24881994
- PMCID: PMC4042017
- DOI: 10.1016/S0140-6736(14)60685-1
Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people
Abstract
Background: The associations of blood pressure with the different manifestations of incident cardiovascular disease in a contemporary population have not been compared. In this study, we aimed to analyse the associations of blood pressure with 12 different presentations of cardiovascular disease.
Methods: We used linked electronic health records from 1997 to 2010 in the CALIBER (CArdiovascular research using LInked Bespoke studies and Electronic health Records) programme to assemble a cohort of 1·25 million patients, 30 years of age or older and initially free from cardiovascular disease, a fifth of whom received blood pressure-lowering treatments. We studied the heterogeneity in the age-specific associations of clinically measured blood pressure with 12 acute and chronic cardiovascular diseases, and estimated the lifetime risks (up to 95 years of age) and cardiovascular disease-free life-years lost adjusted for other risk factors at index ages 30, 60, and 80 years. This study is registered at ClinicalTrials.gov, number NCT01164371.
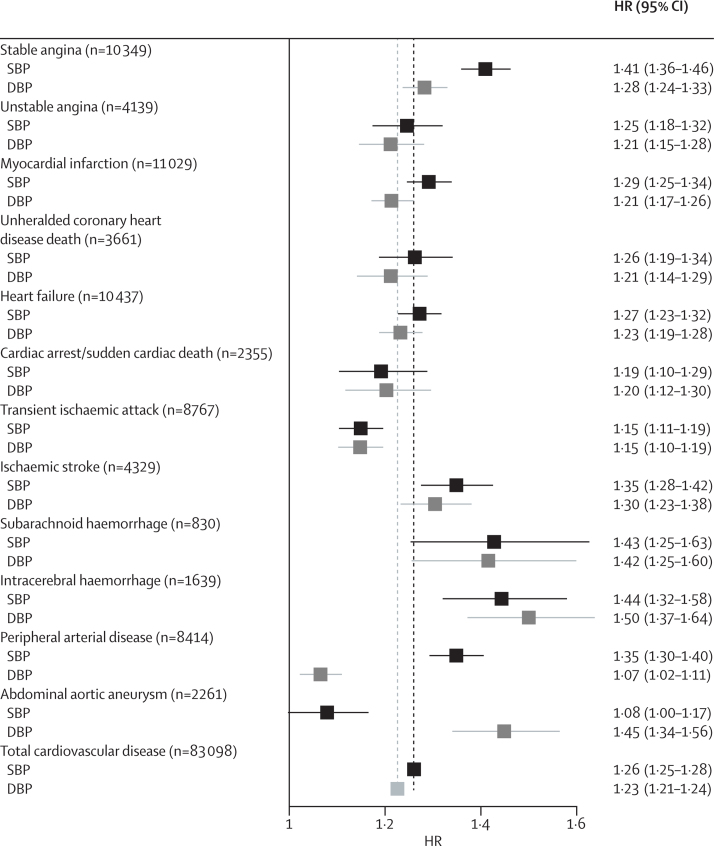
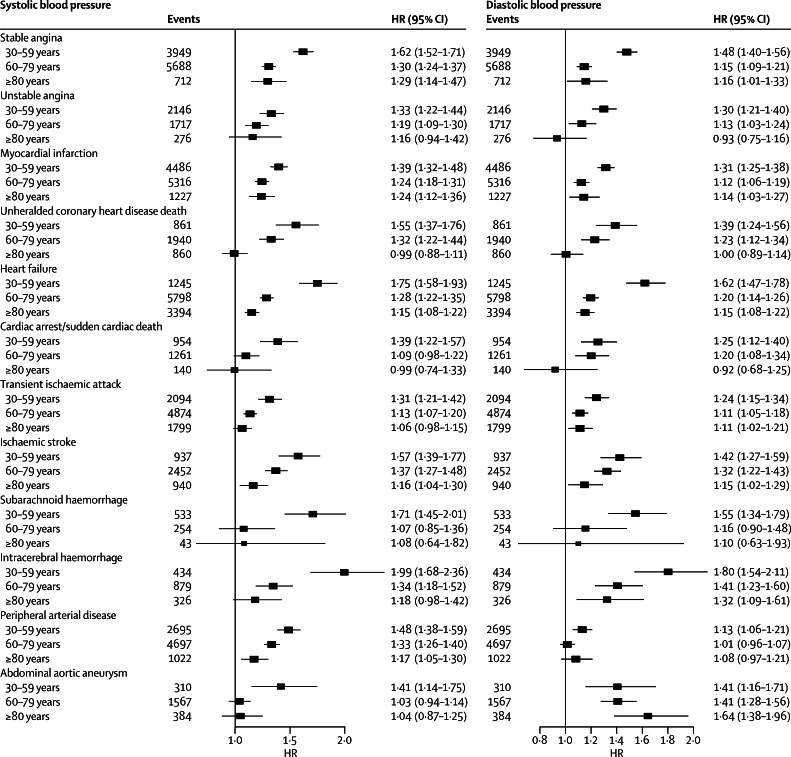
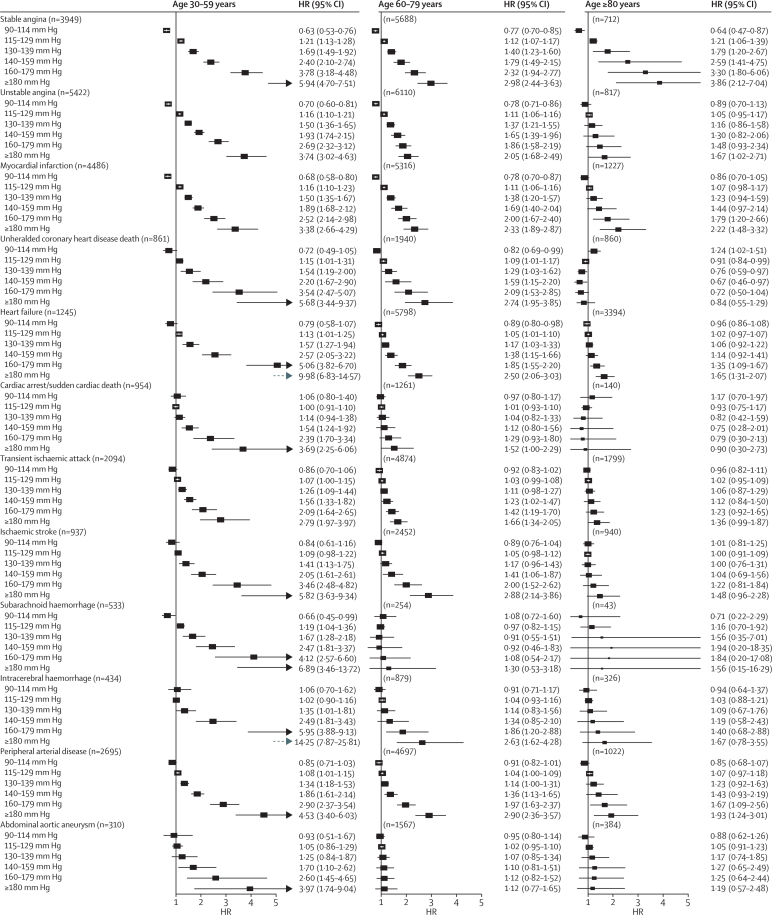
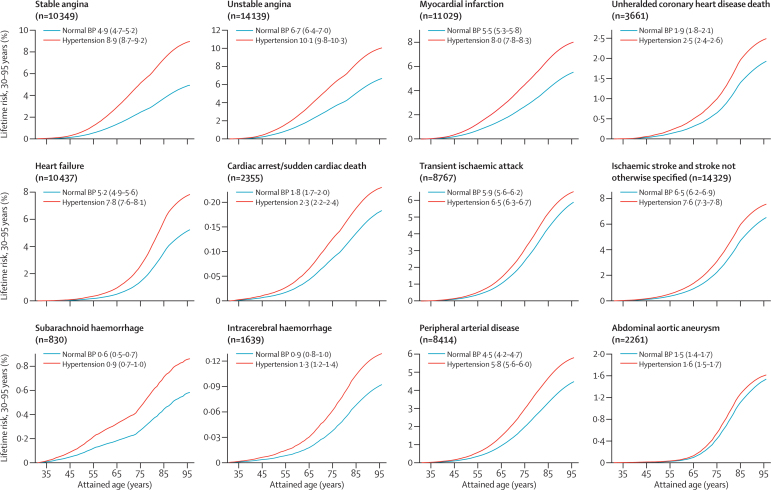
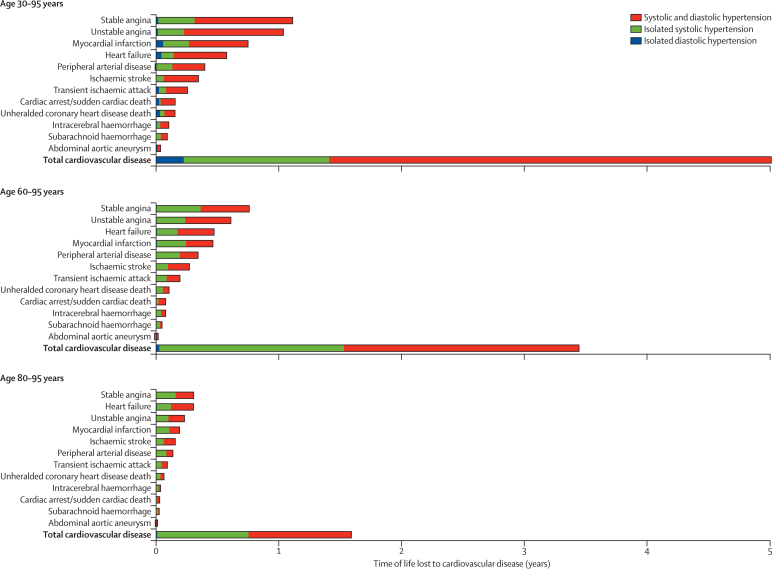
Findings: During 5·2 years median follow-up, we recorded 83,098 initial cardiovascular disease presentations. In each age group, the lowest risk for cardiovascular disease was in people with systolic blood pressure of 90-114 mm Hg and diastolic blood pressure of 60-74 mm Hg, with no evidence of a J-shaped increased risk at lower blood pressures. The effect of high blood pressure varied by cardiovascular disease endpoint, from strongly positive to no effect. Associations with high systolic blood pressure were strongest for intracerebral haemorrhage (hazard ratio 1·44 [95% CI 1·32-1·58]), subarachnoid haemorrhage (1·43 [1·25-1·63]), and stable angina (1·41 [1·36-1·46]), and weakest for abdominal aortic aneurysm (1·08 [1·00-1·17]). Compared with diastolic blood pressure, raised systolic blood pressure had a greater effect on angina, myocardial infarction, and peripheral arterial disease, whereas raised diastolic blood pressure had a greater effect on abdominal aortic aneurysm than did raised systolic pressure. Pulse pressure associations were inverse for abdominal aortic aneurysm (HR per 10 mm Hg 0·91 [95% CI 0·86-0·98]) and strongest for peripheral arterial disease (1·23 [1·20-1·27]). People with hypertension (blood pressure ≥140/90 mm Hg or those receiving blood pressure-lowering drugs) had a lifetime risk of overall cardiovascular disease at 30 years of age of 63·3% (95% CI 62·9-63·8) compared with 46·1% (45·5-46·8) for those with normal blood pressure, and developed cardiovascular disease 5·0 years earlier (95% CI 4·8-5·2). Stable and unstable angina accounted for most (43%) of the cardiovascular disease-free years of life lost associated with hypertension from index age 30 years, whereas heart failure and stable angina accounted for the largest proportion (19% each) of years of life lost from index age 80 years.
Interpretation: The widely held assumptions that blood pressure has strong associations with the occurrence of all cardiovascular diseases across a wide age range, and that diastolic and systolic associations are concordant, are not supported by the findings of this high-resolution study. Despite modern treatments, the lifetime burden of hypertension is substantial. These findings emphasise the need for new blood pressure-lowering strategies, and will help to inform the design of randomised trials to assess them.
Funding: Medical Research Council, National Institute for Health Research, and Wellcome Trust.
Copyright © 2014 Rapsomaniki et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Focus on blood pressure as a major risk factor.Lancet. 2014 May 31;383(9932):1866-8. doi: 10.1016/S0140-6736(14)60896-5. Lancet. 2014. PMID: 24881978 No abstract available.
-
Hypertension. Age-specificity of blood-pressure-associated complications.Nat Rev Cardiol. 2014 Sep;11(9):499-501. doi: 10.1038/nrcardio.2014.109. Epub 2014 Jul 29. Nat Rev Cardiol. 2014. PMID: 25072909
-
[Blood pressure and incidence of 12 cardiovascular diseases: Risks throughout life, life years lost and relationship between different age groups in 1.25 nillion people].Semergen. 2015 Jan-Feb;41(1):50-1. doi: 10.1016/j.semerg.2014.07.014. Epub 2014 Sep 16. Semergen. 2015. PMID: 25239888 Spanish. No abstract available.
References
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, the Prospective Studies Collaboration Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. - PubMed
-
- Lloyd-Jones DM, Leip EP, Larson MG, Vasan RS, Levy D. Novel approach to examining first cardiovascular events after hypertension onset. Hypertension. 2005;45:39–45. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- G9521010/MRC_/Medical Research Council/United Kingdom
- 086091/Z/08/Z/WT_/Wellcome Trust/United Kingdom
- BHF_/British Heart Foundation/United Kingdom
- G0902393/99558/MRC_/Medical Research Council/United Kingdom
- 0938/30/Z/10/Z/WT_/Wellcome Trust/United Kingdom
- MC_PC_13090/MRC_/Medical Research Council/United Kingdom
- 093830/WT_/Wellcome Trust/United Kingdom
- MR/K006584/1/WT_/Wellcome Trust/United Kingdom
- MR/K006584/1/MRC_/Medical Research Council/United Kingdom
- DRF-2009-02-50/DH_/Department of Health/United Kingdom
- MC_U105260558/MRC_/Medical Research Council/United Kingdom
- U10526055/MRC_/Medical Research Council/United Kingdom
- RP-PG-0407-10314/DH_/Department of Health/United Kingdom
- 098504/WT_/Wellcome Trust/United Kingdom
- ARC_/Arthritis Research UK/United Kingdom
- CSO_/Chief Scientist Office/United Kingdom
- G0902393/MRC_/Medical Research Council/United Kingdom
- CRUK_/Cancer Research UK/United Kingdom
- U105260558/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
