

Challenges in diagnosing narcolepsy without cataplexy: a consensus statement
- PMID: 24882898
- PMCID: PMC4015377
- DOI: 10.5665/sleep.3756
Challenges in diagnosing narcolepsy without cataplexy: a consensus statement
Abstract
Background: Diagnosing narcolepsy without cataplexy is often a challenge as the symptoms are nonspecific, current diagnostic tests are limited, and there are no useful biomarkers. In this report, we review the clinical and physiological aspects of narcolepsy without cataplexy, the limitations of available diagnostic procedures, and the differential diagnoses, and we propose an approach for more accurate diagnosis of narcolepsy without cataplexy.
Methods: A group of clinician-scientists experienced in narcolepsy reviewed the literature and convened to discuss current diagnostic tools, and to map out directions for research that should lead to a better understanding and more accurate diagnosis of narcolepsy without cataplexy.
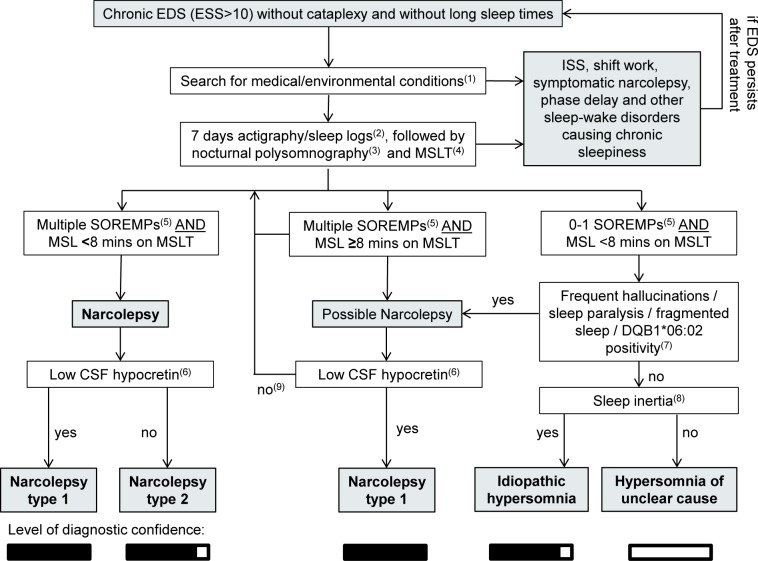
Recommendations: To aid in the identification of narcolepsy without cataplexy, we review key indicators of narcolepsy and present a diagnostic algorithm. A detailed clinical history is mainly helpful to rule out other possible causes of chronic sleepiness. The multiple sleep latency test remains the most important measure, and prior sleep deprivation, shift work, or circadian disorders should be excluded by actigraphy or sleep logs. A short REM sleep latency (≤ 15 minutes) on polysomnography can aid in the diagnosis of narcolepsy without cataplexy, although sensitivity is low. Finally, measurement of hypocretin levels can helpful, as levels are low to intermediate in 10% to 30% of narcolepsy without cataplexy patients.
Keywords: insomnia; multiple sleep latency test; narcolepsy; polysomnography.
Figures
References
-
- Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol. 2002;59:1553–62. - PubMed
-
- Singh M, Drake CL, Roth T. The prevalence of multiple sleep-onset REM periods in a population-based sample. Sleep. 2006;29:890–5. - PubMed
-
- Mignot E, Lin L, Finn L, Lopes C, Pluff K, Sundstrom ML, Young T. Correlates of sleep-onset REM periods during the multiple sleep latency test in community adults. Brain. 2006;129:1609–23. - PubMed
-
- Luca G, Haba-Rubio J, Dauvilliers Y, et al. European Narcolepsy Network (EU-NN) Clinical, polysomnographic and genome-wide association analyses of narcolepsy with cataplexy: a European Narcolepsy Network study. J Sleep Res. 2013;22:482–95. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
