

Safety and efficacy of protease inhibitor based combination therapy in a single-center "real-life" cohort of 110 patients with chronic hepatitis C genotype 1 infection
- PMID: 24884400
- PMCID: PMC4102246
- DOI: 10.1186/1471-230X-14-87
Safety and efficacy of protease inhibitor based combination therapy in a single-center "real-life" cohort of 110 patients with chronic hepatitis C genotype 1 infection
Abstract
Background: The combination of boceprevir or telaprevir with peginterferon-alfa and ribavirin for the treatment of patients infected with HCV genotype 1 has led to significantly increased rates of sustained virological response (SVR) in phase III trials. There is only limited data regarding the safety and efficacy in a "real-life" cohort.
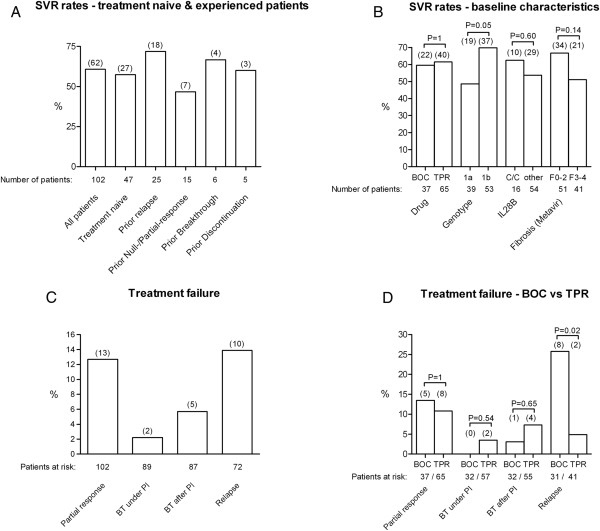
Methods: We analyzed a cohort of 110 unselected HCV patients who started triple therapy from September 2011 to February 2013 by chart review with focus on the individual course of treatment, complications and outcome. We excluded 8 patients from analysis because of HIV-coinfection (N = 6) or status post liver transplant (N = 2). Importantly, 41 patients displayed F3 or F4 fibrosis, 10 patients had a history of treatment with protease/polymerase inhibitors and 15 patients were prior partial- or null-responder.
Results: SVR12 was achieved in 62 of the 102 patients (60.8%). A high rate of serious adverse events (N = 30) was observed in 22 patients including 2 fatalities in cirrhotic diabetes patients. Age >50 years, liver cirrhosis, bilirubin >1.1 mg/dl (P < 0.01, each), platelets <100,000/μl (P = 0.01), ASAT >100 U/l (P = 0.03) and albumin ≤35 g/l (P = 0.04) at baseline were associated with occurence of a SAE.
Conclusions: The frequency of SVR in a "real-life" treatment setting is slightly lower as compared to the results of the phase III trials for telaprevir or boceprevir. Importantly, we observed a high frequency of SAE in triple therapy, especially in patients with liver cirrhosis.
Figures
Similar articles
-
Effectiveness of telaprevir or boceprevir in treatment-experienced patients with HCV genotype 1 infection and cirrhosis.Gastroenterology. 2014 Jul;147(1):132-142.e4. doi: 10.1053/j.gastro.2014.03.051. Epub 2014 Apr 3. Gastroenterology. 2014. PMID: 24704719
-
Favourable SVR12 rates with boceprevir or telaprevir triple therapy in HIV/HCV coinfected patients.Neth J Med. 2015 Aug;73(7):324-30. Neth J Med. 2015. PMID: 26314715
-
A US multicenter study of hepatitis C treatment of liver transplant recipients with protease-inhibitor triple therapy.J Hepatol. 2014 Sep;61(3):508-14. doi: 10.1016/j.jhep.2014.04.037. Epub 2014 May 5. J Hepatol. 2014. PMID: 24801415 Free PMC article.
-
Impact of HCV protease-inhibitor-based triple therapy for chronic HCV genotype 1 infection.Antivir Ther. 2011;16(8):1187-201. doi: 10.3851/IMP1934. Antivir Ther. 2011. PMID: 22155901 Review.
-
Telaprevir: a review of its use in the management of genotype 1 chronic hepatitis C.Drugs. 2012 Mar 26;72(5):619-41. doi: 10.2165/11208370-000000000-00000. Drugs. 2012. PMID: 22439668 Review.
Cited by
-
Effectiveness research in the evolving HCV landscape.Dig Dis Sci. 2014 Dec;59(12):2845-7. doi: 10.1007/s10620-014-3345-6. Dig Dis Sci. 2014. PMID: 25190262 No abstract available.
-
Final Results of the Telaprevir Access Program: FibroScan Values Predict Safety and Efficacy in Hepatitis C Patients with Advanced Fibrosis or Cirrhosis.PLoS One. 2015 Sep 23;10(9):e0138503. doi: 10.1371/journal.pone.0138503. eCollection 2015. PLoS One. 2015. PMID: 26398503 Free PMC article. Clinical Trial.
-
Effectiveness and safety of first-generation protease inhibitors in real-world patients with hepatitis C virus genotype 1 infection in Brazil: a multicenter study.Clinics (Sao Paulo). 2017 Jun;72(6):378-385. doi: 10.6061/clinics/2017(06)08. Clinics (Sao Paulo). 2017. PMID: 28658438 Free PMC article. Clinical Trial.
-
[Hepatitis C in prisons : Treatment and barriers to the elimination goals of the United Nations].Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2024 Jan;67(1):36-44. doi: 10.1007/s00103-023-03808-y. Epub 2023 Dec 28. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2024. PMID: 38155308 Free PMC article. German.
-
Predictors of early treatment discontinuation and severe anemia in a Brazilian cohort of hepatitis C patients treated with first-generation protease inhibitors.Braz J Med Biol Res. 2016 Jun 23;49(7):e5300. doi: 10.1590/1414-431X20165300. Braz J Med Biol Res. 2016. PMID: 27356107 Free PMC article.
References
-
- Global surveillance and control of hepatitis C: report of a WHO consultation organized in collaboration with the viral hepatitis prevention board, Antwerp, Belgium. J Viral Hepat. 1999;6:35–47. - PubMed
-
- Poordad F, McCone J, Bacon BR, Bruno S, Manns MP, Sulkowski MS, Jacobson IM, Reddy KR, Goodman ZD, Boparai N, DuNubile MJ, Sniukiene V, Brass CA, Albrecht JK, Bronowicki JP. Boceprevir for untreated chronic HCV genotype 1-infection. N Engl J Med. 2011;364:1195–206. doi: 10.1056/NEJMoa1010494. - DOI - PMC - PubMed
-
- Jacobson IM, McHutchison JG, Dusheiko G, Di Bisceglie AM, Reddy KR, Bzowej NH, Marcellin P, Muir AJ, Ferenci P, Flisiak R, George J, Rizzetto M, Shouval D, Sola R, Terg RA, Yoshida EM, Adda N, Bengtsson L, Sankoh AJ, Kieffer TL, George S, Kauffman RS, Zeuzem S. Telaprevir for previously untreated chronic hepatitis C virus infection. N Engl J Med. 2011;364:2405–16. doi: 10.1056/NEJMoa1012912. - DOI - PubMed
-
- Sherman KE, Flamm SL, Afdhal NH, Nelson DR, Sulkowski MS, Everson GT, Fried MW, Adler M, Reesink HW, Martin M, Sankoh AJ, Adda N, Kauffman RS, George S, Wright CI, Poordad F. Response-guided telaprevir combination treatment for hepatitis C virus infection. N Engl J Med. 2011;365:1014–24. doi: 10.1056/NEJMoa1014463. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
