

Predicting red blood cell transfusion in hospitalized patients: role of hemoglobin level, comorbidities, and illness severity
- PMID: 24884605
- PMCID: PMC4101854
- DOI: 10.1186/1472-6963-14-213
Predicting red blood cell transfusion in hospitalized patients: role of hemoglobin level, comorbidities, and illness severity
Abstract
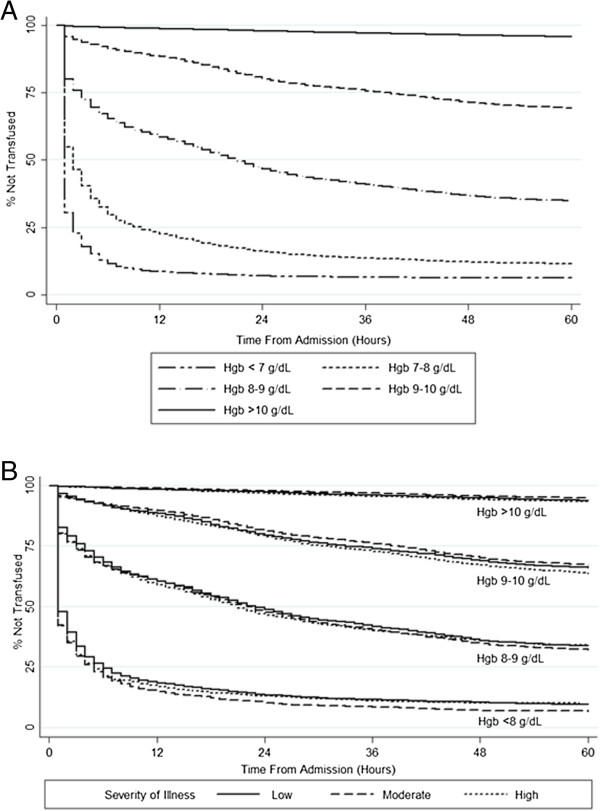
Background: Randomized controlled trial evidence supports a restrictive strategy of red blood cell (RBC) transfusion, but significant variation in clinical transfusion practice persists. Patient characteristics other than hemoglobin levels may influence the decision to transfuse RBCs and explain some of this variation. Our objective was to evaluate the role of patient comorbidities and severity of illness in predicting inpatient red blood cell transfusion events.
Methods: We developed a predictive model of inpatient RBC transfusion using comprehensive electronic medical record (EMR) data from 21 hospitals over a four year period (2008-2011). Using a retrospective cohort study design, we modeled predictors of transfusion events within 24 hours of hospital admission and throughout the entire hospitalization. Model predictors included administrative data (age, sex, comorbid conditions, admission type, and admission diagnosis), admission hemoglobin, severity of illness, prior inpatient RBC transfusion, admission ward, and hospital.
Results: The study cohort included 275,874 patients who experienced 444,969 hospitalizations. The 24 hour and overall inpatient RBC transfusion rates were 7.2% and 13.9%, respectively. A predictive model for transfusion within 24 hours of hospital admission had a C-statistic of 0.928 and pseudo-R2 of 0.542; corresponding values for the model examining transfusion through the entire hospitalization were 0.872 and 0.437. Inclusion of the admission hemoglobin resulted in the greatest improvement in model performance relative to patient comorbidities and severity of illness.
Conclusions: Data from electronic medical records at the time of admission predicts with very high likelihood the incidence of red blood transfusion events in the first 24 hours and throughout hospitalization. Patient comorbidities and severity of illness on admission play a small role in predicting the likelihood of RBC transfusion relative to the admission hemoglobin.
Figures
References
-
- Wass CT, Long TR, Faust RJ, Yaszemski MJ, Joyner MJ. Changes in red blood cell transfusion practice during the past two decades: a retrospective analysis, with the Mayo database, of adult patients undergoing major spine surgery. Transfusion. 2007 Jun;14(6):1022–1027. doi: 10.1111/j.1537-2995.2007.01231.x. - DOI - PubMed
-
- Rana R, Afessa B, Keegan MT, Whalen FX, Nuttall GA, Evenson LK, Peters SG, Winters JL, Hubmayr RD, Moore SB, Gajic O. Evidence-based red cell transfusion in the critically ill: quality improvement using computerized physician order entry. Crit Care Med. 2006;14:7. - PubMed
-
- Vincent JL, Baron JF, Reinhart K, Gattinoni L, Thijs L, Webb A, Meier-Hellmann A, Nollet G, Peres-Bota D. ABC (Anemia and Blood Transfusion in Critical Care) Investigators. Anemia and blood transfusion in critically ill patients. JAMA. 2002;14:1499–1507. doi: 10.1001/jama.288.12.1499. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
