

Fibrinogen concentrate administration attributes to significant reductions of blood loss and transfusion requirements in thoracic aneurysm repair
- PMID: 24884627
- PMCID: PMC4067735
- DOI: 10.1186/1749-8090-9-90
Fibrinogen concentrate administration attributes to significant reductions of blood loss and transfusion requirements in thoracic aneurysm repair
Abstract
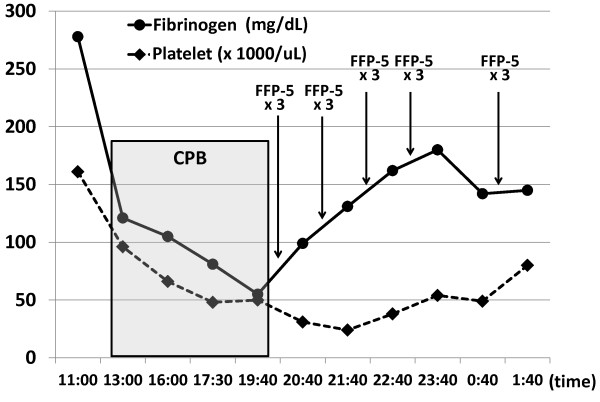
Background: Repair of thoracic aortic aneurysm (TAA) is often associated with massive hemorrhage aggravated by dilutional coagulopathy with severe hypofibrinogenemia. Although only fresh frozen plasma (FFP) is available for acquired hypofibrinogenemia in Japan, the hemostatic effect of FFP has not been enough for dilutional coagulopathy in TAA surgery. There are increasing reports suggesting that fibrinogen concentrate may be effective in controlling perioperative bleeding and reducing transfusion requirements.
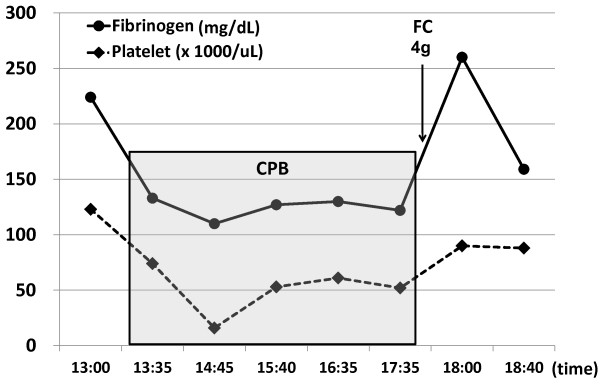
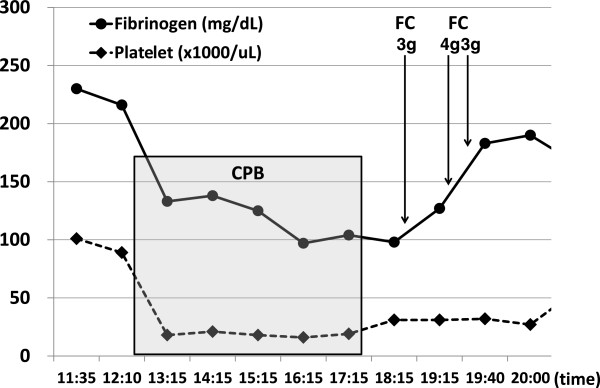
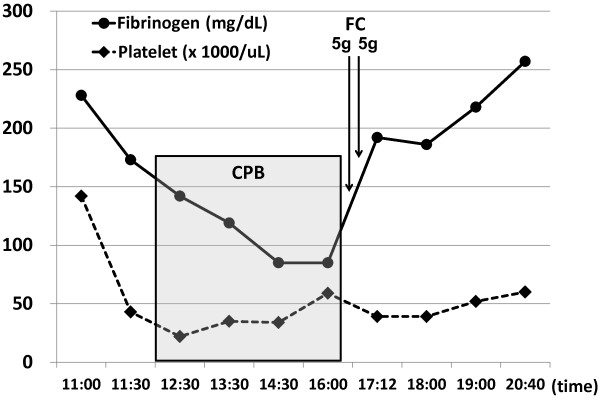
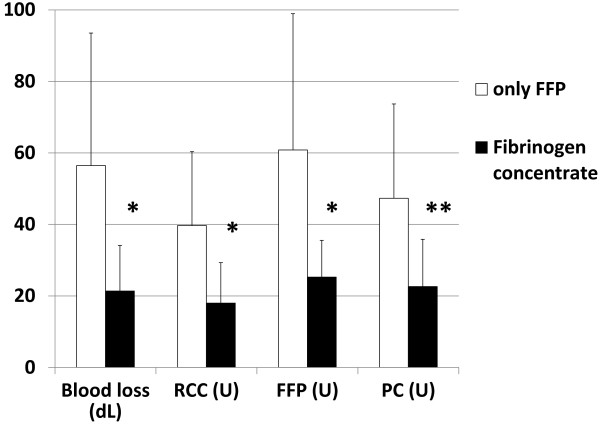
Methods: We retrospectively analyzed the hemostatic effect of fibrinogen concentrate compared with FFP in total 49 cases of elective TAA surgery. In 25 patients, fibrinogen concentrate was administered when the fibrinogen level was below 150 mg/dL at the cardiopulmonary bypass (CPB) termination. The recovery of fibrinogen level, blood loss, and transfused units during surgery were compared between cases of this agent and FFP (n = 24).
Results: We observed rapid increases in plasma fibrinogen level and subsequent improvement in hemostasis by administration of fibrinogen concentrate after CPB termination. The average volume of total blood loss decreased by 64% and the average number of transfused units was reduced by 58% in cases of fibrinogen concentrate given, in comparison with cases of only FFP transfused for fibrinogen supplementation.
Conclusions: In patients showing severe hypofibrinogenemia during TAA surgery, timely administration of fibrinogen concentrate just after removal from CPB is effective for hemostasis, and therefore in reducing blood loss and transfused volumes.
Figures
Similar articles
-
[Required laboratory examination and blood transfusion therapy in massive hemorrhage during surgery].Rinsho Byori. 2011 Jul;59(7):678-83. Rinsho Byori. 2011. PMID: 21874794 Review. Japanese.
-
Thromboelastometry-guided administration of fibrinogen concentrate for the treatment of excessive intraoperative bleeding in thoracoabdominal aortic aneurysm surgery.J Thorac Cardiovasc Surg. 2009 Sep;138(3):694-702. doi: 10.1016/j.jtcvs.2008.11.065. Epub 2009 May 17. J Thorac Cardiovasc Surg. 2009. PMID: 19698858
-
Fibrinogen concentrate reduces intraoperative bleeding when used as first-line hemostatic therapy during major aortic replacement surgery: results from a randomized, placebo-controlled trial.J Thorac Cardiovasc Surg. 2013 Mar;145(3 Suppl):S178-85. doi: 10.1016/j.jtcvs.2012.12.083. J Thorac Cardiovasc Surg. 2013. PMID: 23410777 Clinical Trial.
-
Effects of Fibrinogen Concentrate Supplementation on Postoperative Bleeding in Infants Undergoing Complex Cardiac Surgery.Pediatr Cardiol. 2025 Jun;46(5):1381-1389. doi: 10.1007/s00246-024-03559-w. Epub 2024 Jul 9. Pediatr Cardiol. 2025. PMID: 38980325
-
Fibrinogen for the management of critical obstetric hemorrhage.J Obstet Gynaecol Res. 2019 Jan;45(1):13-21. doi: 10.1111/jog.13788. Epub 2018 Aug 28. J Obstet Gynaecol Res. 2019. PMID: 30155944 Free PMC article. Review.
Cited by
-
Accelerated activation of the coagulation pathway during cardiopulmonary bypass in aortic replacement surgery: a prospective observational study.J Cardiothorac Surg. 2015 Jun 23;10:84. doi: 10.1186/s13019-015-0295-9. J Cardiothorac Surg. 2015. PMID: 26099510 Free PMC article.
-
Insufficient fibrinogen response following free flap surgery is associated with bleeding complications.GMS Interdiscip Plast Reconstr Surg DGPW. 2016 Nov 22;5:Doc22. doi: 10.3205/iprs000101. eCollection 2016. GMS Interdiscip Plast Reconstr Surg DGPW. 2016. PMID: 27975041 Free PMC article.
-
The hemostatic disturbance in patients with acute aortic dissection: A prospective observational study.Medicine (Baltimore). 2016 Sep;95(36):e4710. doi: 10.1097/MD.0000000000004710. Medicine (Baltimore). 2016. PMID: 27603366 Free PMC article.
-
Preoperative fibrinogen before the repair of type A aortic dissection: Are the results too good to be true?: Editorial comment on: Li J, Wu Q, Tang M, Shen Y, Qiu Z, Chen X, Chen X, Chen L. Preoperative clinical application of human fibrinogen in patients with acute Stanford type A aortic dissection: A single-center retrospective study. Journal of Cardiac Surgery. In press.J Card Surg. 2022 Oct;37(10):3166-3167. doi: 10.1111/jocs.16760. Epub 2022 Jul 21. J Card Surg. 2022. PMID: 35864816 Free PMC article. No abstract available.
-
Early administration of fibrinogen concentrates improves the short-term outcomes of severe pelvic fracture patients.Acute Med Surg. 2017 Apr 2;4(3):271-277. doi: 10.1002/ams2.268. eCollection 2017 Jul. Acute Med Surg. 2017. PMID: 29123874 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
