

Effectiveness of the Chest Pain Choice decision aid in emergency department patients with low-risk chest pain: study protocol for a multicenter randomized trial
- PMID: 24884807
- PMCID: PMC4031497
- DOI: 10.1186/1745-6215-15-166
Effectiveness of the Chest Pain Choice decision aid in emergency department patients with low-risk chest pain: study protocol for a multicenter randomized trial
Abstract
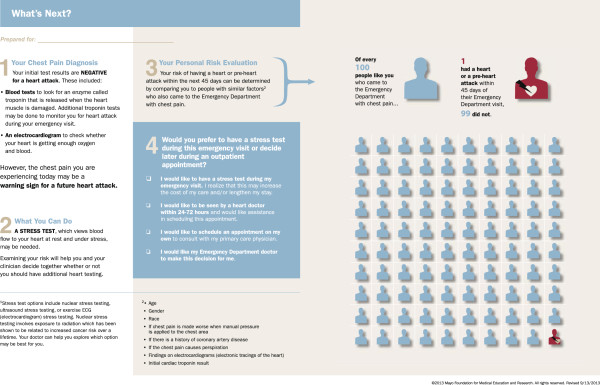
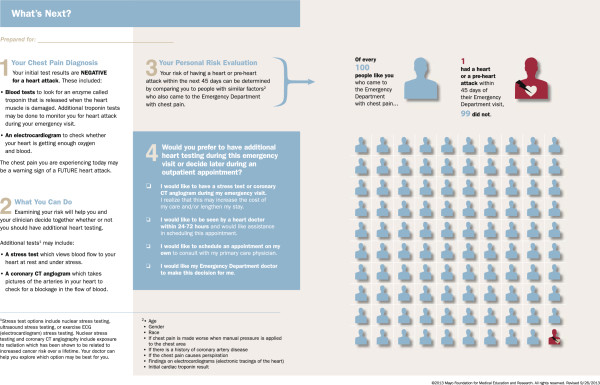
Background: Chest pain is the second most common reason patients visit emergency departments (EDs) and often results in very low-risk patients being admitted for prolonged observation and advanced cardiac testing. Shared decision-making, including educating patients regarding their 45-day risk for acute coronary syndrome (ACS) and management options, might safely decrease healthcare utilization.
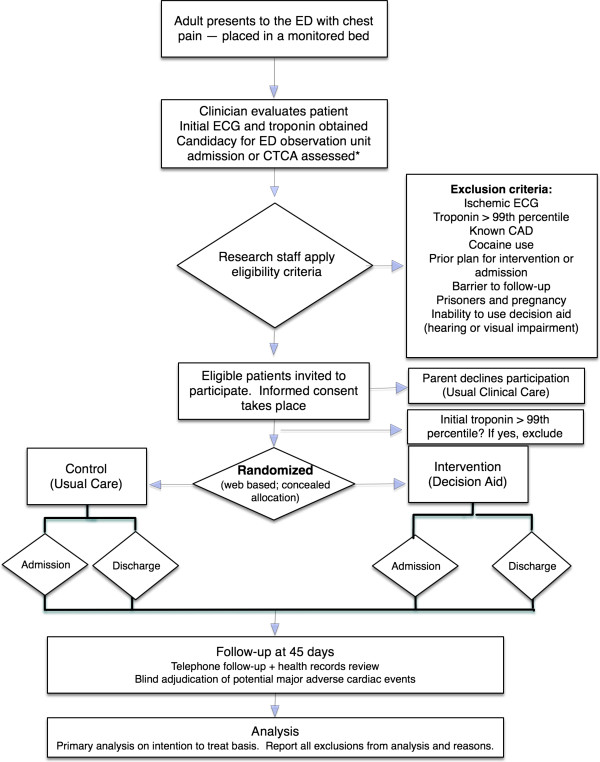
Methods/design: This is a protocol for a multicenter practical patient-level randomized trial to compare an intervention group receiving a decision aid, Chest Pain Choice (CPC), to a control group receiving usual care. Adults presenting to five geographically and ethnically diverse EDs who are being considered for admission for observation and advanced cardiac testing will be eligible for enrollment. We will measure the effect of CPC on (1) patient knowledge regarding their 45-day risk for ACS and the available management options (primary outcome); (2) patient engagement in the decision-making process; (3) the degree of conflict patients experience related to feeling uninformed (decisional conflict); (4) patient and clinician satisfaction with the decision made; (5) the rate of major adverse cardiac events at 30 days; (6) the proportion of patients admitted for advanced cardiac testing; and (7) healthcare utilization. To assess these outcomes, we will administer patient and clinician surveys immediately after each clinical encounter, obtain video recordings of the patient-clinician discussion, administer a patient healthcare utilization diary, analyze hospital billing records, review the electronic medical record, and conduct telephone follow-up.
Discussion: This multicenter trial will robustly assess the effectiveness of a decision aid on patient-centered outcomes, safety, and healthcare utilization in low-risk chest pain patients from a variety of geographically and ethnically diverse EDs.
Trial registration: NCT01969240.
Figures
References
-
- Niska R, Bhuiya F, Xu J. National hospital ambulatory medical care survey, emergency department summary. Natl Health Stat Rep. 2007;2010(26):1–31. - PubMed
-
- Healthcare utilization project statistical brief #26. Hospital stays for circulatory diseases. Rockville, Maryland, USA: Agency for healthcare research and quality; 2004. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb26.pdf. - PubMed
-
- Mitchell AM, Garvey JL, Chandra A, Diercks D, Pollack CV, Kline JA. Prospective multicenter study of quantitative pretest probability assessment to exclude acute coronary syndrome for patients evaluated in emergency department chest pain units. Ann Emerg Med. 2006;47(5):447. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
