

Urinary soluble urokinase receptor levels are elevated and pathogenic in patients with primary focal segmental glomerulosclerosis
- PMID: 24884842
- PMCID: PMC4064821
- DOI: 10.1186/1741-7015-12-81
Urinary soluble urokinase receptor levels are elevated and pathogenic in patients with primary focal segmental glomerulosclerosis
Abstract
Background: Focal segmental glomerulosclerosis (FSGS) is a major cause of end-stage renal disease. Recent studies have proposed that plasma soluble urokinase receptor (suPAR) might be a causative circulating factor but this proposal has caused controversy. This study aimed to measure urinary suPAR levels in patients with primary FSGS and its significance in the pathogenesis of FSGS.
Methods: Sixty-two patients with primary FSGS, diagnosed between January 2006 and January 2012, with complete clinical and pathologic data were enrolled, together with disease and normal controls. Urinary suPAR levels were measured using commercial ELISA kits and were corrected by urinary creatinine (Cr). The associations between urinary suPAR levels and clinical data at presentation and during follow up were analyzed. Conditionally immortalized human podocytes were used to study the effect of urinary suPAR on activating β3 integrin detected by AP5 staining.
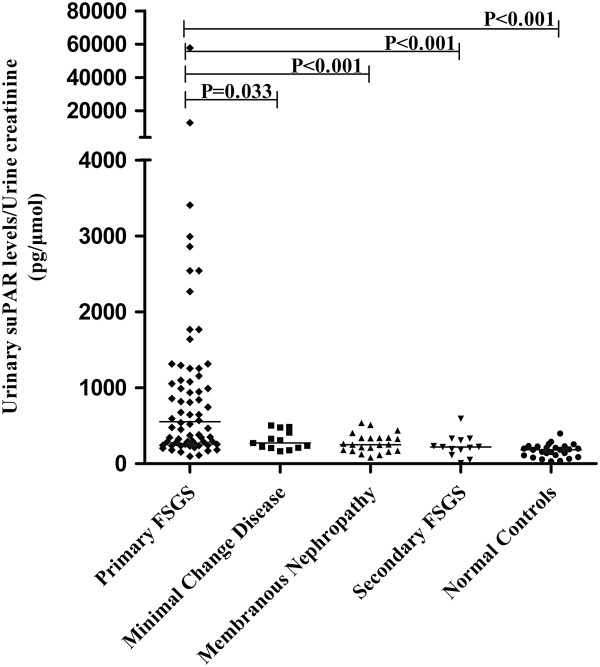
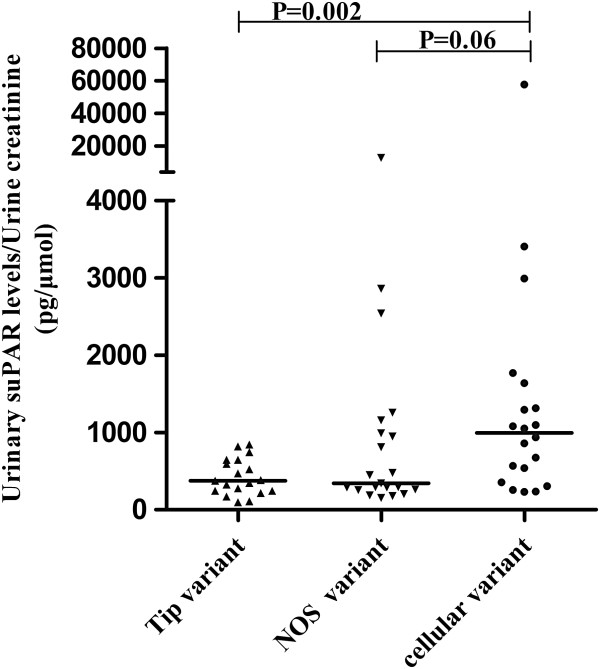
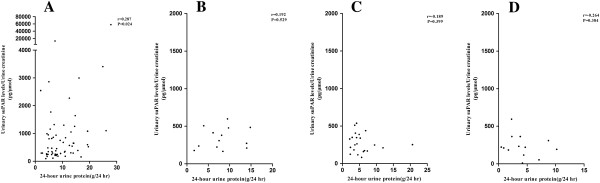
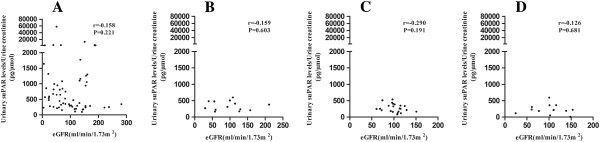
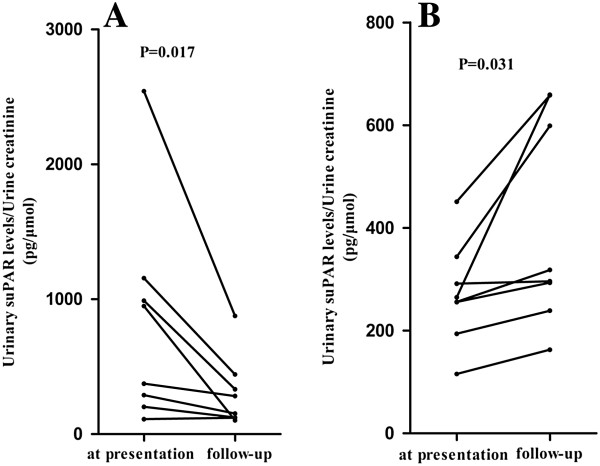
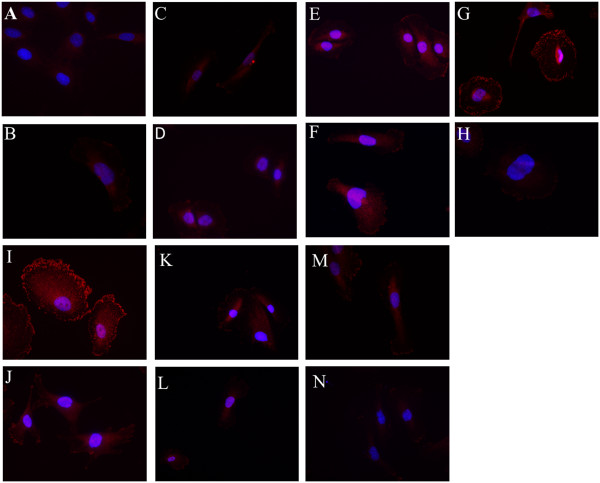
Results: The urinary suPAR level of patients with primary FSGS (500.56, IQR 262.78 to 1,059.44 pg/μmol Cr) was significantly higher than that of patients with minimal change disease (307.86, IQR 216.54 to 480.18 pg/μmol Cr, P = 0.033), membranous nephropathy (250.23, IQR 170.37 to 357.59 pg/μmol Cr, P <0.001), secondary FSGS (220.45, IQR 149.38 to 335.54 pg/μmol Cr, P <0.001) and normal subjects (183.59, IQR 103.92 to 228.78 pg/μmol Cr, P <0.001). The urinary suPAR level of patients with cellular variant was significantly higher than that of patients with tip variant. The urinary suPAR level in the patients with primary FSGS was positively correlated with 24-hour urine protein (r = 0.287, P = 0.024). During follow up, the urinary suPAR level of patients with complete remission decreased significantly (661.19, IQR 224.32 to 1,115.29 pg/μmol Cr versus 217.68, IQR 121.77 to 415.55 pg/μmol Cr, P = 0.017). The AP5 signal was strongly induced along the cell membrane when human differentiated podocytes were incubated with the urine of patients with FSGS at presentation, and the signal could be reduced by a blocking antibody specific to uPAR.
Conclusions: Urinary suPAR was specifically elevated in patients with primary FSGS and was associated with disease severity. The elevated urinary suPAR could activate β3 integrin on human podocytes.
Figures
Comment in
-
suPAR and Team Nephrology.BMC Med. 2014 May 20;12:82. doi: 10.1186/1741-7015-12-82. BMC Med. 2014. PMID: 24885021 Free PMC article.
References
-
- Rich AR. A hitherto undescribed vulnerability of the juxtamedullary glomeruli in lipoid nephrosis. Bull Johns Hopkins Hosp. 1957;100:173–186. - PubMed
-
- Kriz W. The pathogenesis of ‘classic’ focal segmental glomerulosclerosis-lessons from rat models. Nephrol Dial Transplant. 2003;18:vi39–vi44. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
