

Safety of artemether-lumefantrine exposure in first trimester of pregnancy: an observational cohort
- PMID: 24884890
- PMCID: PMC4040412
- DOI: 10.1186/1475-2875-13-197
Safety of artemether-lumefantrine exposure in first trimester of pregnancy: an observational cohort
Abstract
Background: There is limited data available regarding safety profile of artemisinins in early pregnancy. They are, therefore, not recommended by WHO as a first-line treatment for malaria in first trimester due to associated embryo-foetal toxicity in animal studies. The study assessed birth outcome among pregnant women inadvertently exposed to artemether-lumefantrine (AL) during first trimester in comparison to those of women exposed to other anti-malarial drugs or no drug at all during the same period of pregnancy.
Methods: Pregnant women with gestational age <20 weeks were recruited from Maternal Health clinics or from monthly house visits (demographic surveillance), and followed prospectively until delivery.
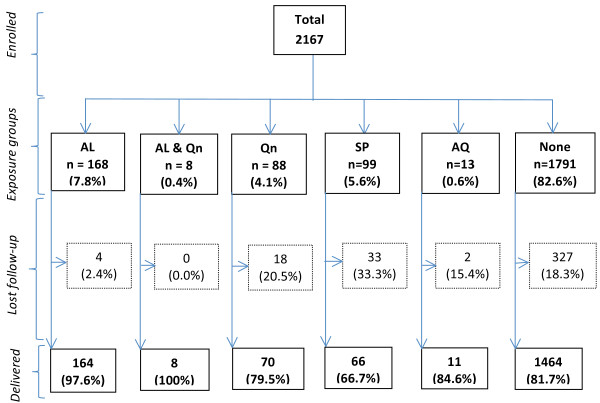
Results: 2167 pregnant women were recruited and 1783 (82.3%) completed the study until delivery. 319 (17.9%) used anti-malarials in first trimester, of whom 172 (53.9%) used (AL), 78 (24.4%) quinine, 66 (20.7%) sulphadoxine-pyrimethamine (SP) and 11 (3.4%) amodiaquine. Quinine exposure in first trimester was associated with an increased risk of miscarriage/stillbirth (OR 2.5; 1.3-5.1) and premature birth (OR 2.6; 1.3-5.3) as opposed to AL with (OR 1.4; 0.8-2.5) for miscarriage/stillbirth and (OR 0.9; 0.5-1.8) for preterm birth. Congenital anomalies were identified in 4 exposure groups namely AL only (1/164[0.6%]), quinine only (1/70[1.4%]), SP (2/66[3.0%]), and non-anti-malarial exposure group (19/1464[1.3%]).
Conclusion: Exposure to AL in first trimester was more common than to any other anti-malarial drugs. Quinine exposure was associated with adverse pregnancy outcomes which was not the case following other anti-malarial intake. Since AL and quinine were used according to their availability rather than to disease severity, it is likely that the effect observed was related to the drug and not to the disease itself. Even with this caveat, a change of policy from quinine to AL for the treatment of uncomplicated malaria during the whole pregnancy period could be already envisaged.
Figures
Similar articles
-
Exposure to artemether-lumefantrine (Coartem) in first trimester pregnancy in an observational study in Zambia.Malar J. 2015 Feb 14;14:77. doi: 10.1186/s12936-015-0578-6. Malar J. 2015. PMID: 25877884 Free PMC article.
-
A systematic review of the safety and efficacy of artemether-lumefantrine against uncomplicated Plasmodium falciparum malaria during pregnancy.Malar J. 2012 May 1;11:141. doi: 10.1186/1475-2875-11-141. Malar J. 2012. PMID: 22548983 Free PMC article.
-
Safety of artemether-lumefantrine in pregnant women with malaria: results of a prospective cohort study in Zambia.Malar J. 2010 Sep 1;9:249. doi: 10.1186/1475-2875-9-249. Malar J. 2010. PMID: 20809964 Free PMC article.
-
Pharmacovigilance of artemether-lumefantrine in pregnant women followed until delivery in Rwanda.Malar J. 2012 Jul 6;11:225. doi: 10.1186/1475-2875-11-225. Malar J. 2012. PMID: 22770264 Free PMC article.
-
Pregnancy outcomes after first-trimester treatment with artemisinin derivatives versus non-artemisinin antimalarials: a systematic review and individual patient data meta-analysis.Lancet. 2023 Jan 14;401(10371):118-130. doi: 10.1016/S0140-6736(22)01881-5. Epub 2022 Nov 25. Lancet. 2023. PMID: 36442488 Free PMC article.
Cited by
-
Usefulness of day 7 lumefantrine plasma concentration as a predictor of malaria treatment outcome in under-fives children treated with artemether-lumefantrine in Tanzania.Malar J. 2020 Feb 11;19(1):66. doi: 10.1186/s12936-020-3150-y. Malar J. 2020. PMID: 32046718 Free PMC article. Clinical Trial.
-
Birth prevalence of neural tube defects in eastern Africa: a systematic review and meta-analysis.BMC Neurol. 2022 Jun 1;22(1):202. doi: 10.1186/s12883-022-02697-z. BMC Neurol. 2022. PMID: 35650541 Free PMC article.
-
A roadmap for understanding sulfadoxine-pyrimethamine in malaria chemoprevention.Parasitology. 2025 Feb;152(2):133-142. doi: 10.1017/S0031182025000071. Parasitology. 2025. PMID: 39844654 Free PMC article. Review.
-
Efficacy and Safety of Artemisinin-Based Combination Therapy for the Treatment of Uncomplicated Malaria in Pregnant Women: A Systematic Review and Meta-Analysis.Ther Clin Risk Manag. 2021 Dec 22;17:1353-1370. doi: 10.2147/TCRM.S336771. eCollection 2021. Ther Clin Risk Manag. 2021. PMID: 35221688 Free PMC article. Review.
-
Risks of miscarriage and inadvertent exposure to artemisinin derivatives in the first trimester of pregnancy: a prospective cohort study in western Kenya.Malar J. 2015 Nov 18;14:461. doi: 10.1186/s12936-015-0950-6. Malar J. 2015. PMID: 26581434 Free PMC article.
References
-
- Steketee RW, Nahlen BL, Parise ME, Menendez C. The burden of malaria in pregnancy in malaria-endemic areas. Am J Trop Med Hyg. 2001;64:28–35. - PubMed
-
- CfDER. Reviewer guidance evaluating the risks of drug exposure in human pregnancies. USA: Food and Drug Administration; 2005.
-
- WHO. Guidelines for the treatment of malaria: second edition. Geneva: World Health Organization; 2010.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
