

Autoimmune pancreatitis can develop into chronic pancreatitis
- PMID: 24884922
- PMCID: PMC4038704
- DOI: 10.1186/1750-1172-9-77
Autoimmune pancreatitis can develop into chronic pancreatitis
Abstract
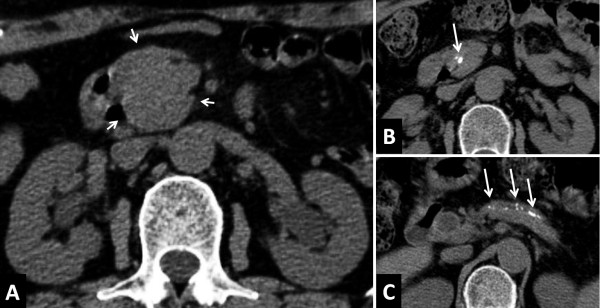
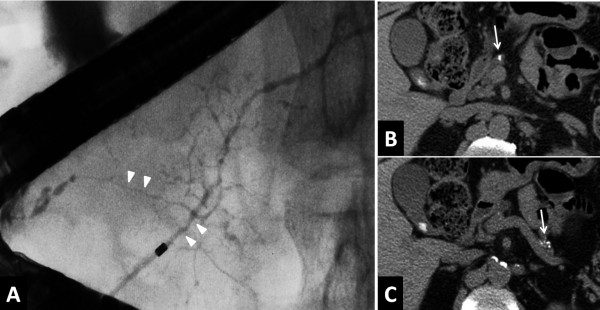
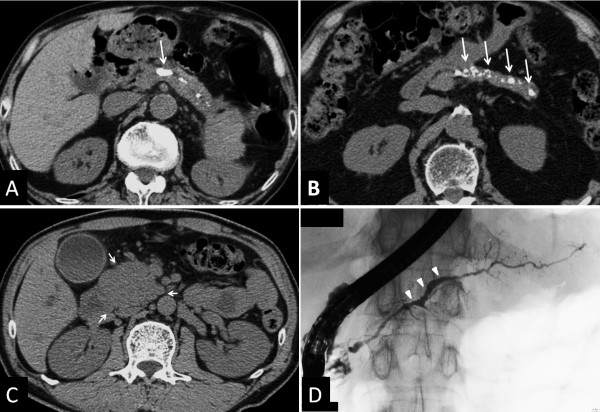
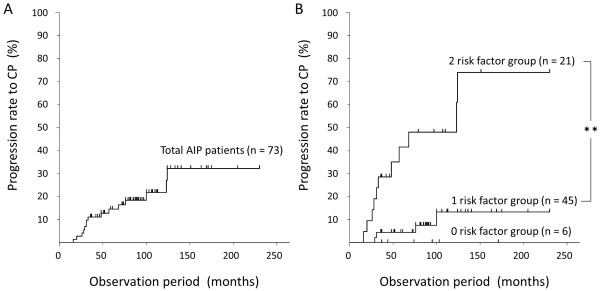
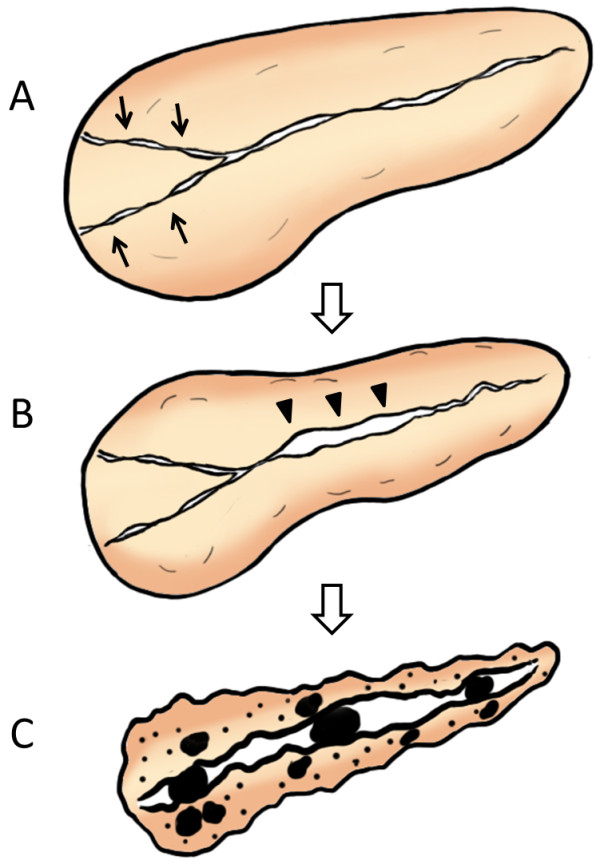
Autoimmune pancreatitis (AIP) has been recognized as a distinct type of pancreatitis that is possibly caused by autoimmune mechanisms. AIP is characterized by high serum IgG4 and IgG4-positive plasma cell infiltration in affected pancreatic tissue. Acute phase AIP responds favorably to corticosteroid therapy and results in the amelioration of clinical findings. However, the long-term prognosis and outcome of AIP remain unclear. We have proposed a working hypothesis that AIP can develop into ordinary chronic pancreatitis resembling alcoholic pancreatitis over a long-term course based on several clinical findings, most notably frequent pancreatic stone formation. In this review article, we describe a series of study results to confirm our hypothesis and clarify that: 1) pancreatic calcification in AIP is closely associated with disease recurrence; 2) advanced stage AIP might have earlier been included in ordinary chronic pancreatitis; 3) approximately 40% of AIP patients experience pancreatic stone formation over a long-term course, for which a primary risk factor is narrowing of both Wirsung's and Santorini's ducts; and 4) nearly 20% of AIP patients progress to confirmed chronic pancreatitis according to the revised Japanese Clinical Diagnostic Criteria, with independent risk factors being pancreatic head swelling and non-narrowing of the pancreatic body duct.
Figures
References
-
- Watanabe T, Yamashita K, Fujikawa S, Sakurai T, Kudo M, Shiokawa M, Kodama Y, Uchida K, Okazaki K, Chiba T. Involvement of activation of toll-like receptors and nucleotide-binding oligomerization domain-like receptors in enhanced IgG4 responses in autoimmune pancreatitis. Arthritis Rheum. 2012;64:914–924. doi: 10.1002/art.33386. - DOI - PubMed
-
- Kawa S, Hamano H, Kiyosawa K. In: The autoimmune diseases. Rose N, MacKay I, editor. St Louis: Academic Press; 2006. Pancreatitis.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
