

Tandem keyhole foraminotomy in the treatment of cervical radiculopathy: retrospective review of 35 cases
- PMID: 24884935
- PMCID: PMC4041334
- DOI: 10.1186/1749-799X-9-38
Tandem keyhole foraminotomy in the treatment of cervical radiculopathy: retrospective review of 35 cases
Abstract
Background: There has been no report regarding the results of two-level keyhole foraminotomy. The purpose of this study was to detail clinical outcomes following consecutive two-level cervical foraminotomy (tandem keyhole foraminotomy (TKF)) in patients with radiculopathy.
Methods: The authors conducted a retrospective review of 35 cases involving patients treated by a single surgeon using TKF. Clinical symptoms, data of physical examinations, pathology and clinical outcomes were detailed and discussed about this surgical method.
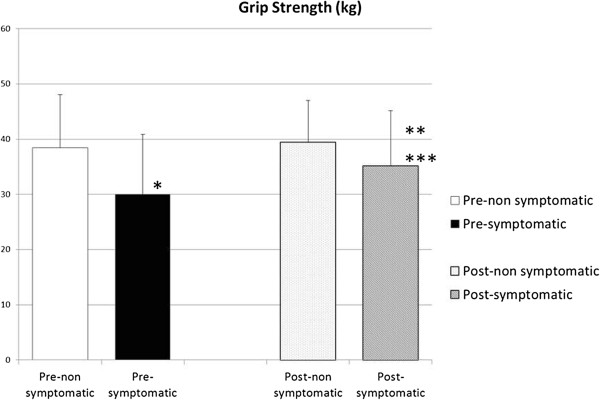
Results: Patients consisted of cervical disc herniation (CDH) (19/35), cervical spondylotic radiculopathy (CSR) (13/35), and cervical spondylotic amyotrophy (CSA) (3/35). TKF was performed from C3 to C5 in 2 patients (6%), from C4 to C6 in 7 patients (20%), from C5 to C7 in 23 patients (66%), and from C6 to T1 in 3 patients (8%). The mean operative duration was 99.2 min (range, 72 to 168 min). The mean estimated blood loss was 55.8 g (range, 0 to 200 g). Radicular pain was relieved within 3 months in 88% (29/32) and in 97% (31/32) at final follow-up. Resolution of muscle weakness was recognized within 6 months after operation in all CSA cases. Sixty-six percent of patients showed a greater than 20% deficit in grip weakness on the affected side compared with the normal side. After pain was relieved, grip strength improved by more than 15%.
Conclusions: TKF is a safe and highly effective procedure for patients with cervical radiculopathy and does not require invasive preoperative examinations. Further investigation is required to determine the effects of consecutive facetectomy.
Figures



Similar articles
-
Minimally Invasive Full-Endoscopic Posterior Cervical Foraminotomy Assisted by O-Arm-Based Navigation.Pain Physician. 2018 May;21(3):E215-E223. Pain Physician. 2018. PMID: 29871377
-
The posterior cervical foraminotomy in the treatment of cervical disc/osteophyte disease: a single-surgeon experience with a minimum of 5 years' clinical and radiographic follow-up.J Neurosurg Spine. 2009 Apr;10(4):347-56. doi: 10.3171/2008.12.SPINE08576. J Neurosurg Spine. 2009. PMID: 19441994
-
Keyhole Foraminotomy via a Percutaneous Posterior Full-endoscopic Approach for Cervical Radiculopathy: An Advanced Procedure and Clinical Study.Curr Med Sci. 2020 Dec;40(6):1170-1176. doi: 10.1007/s11596-020-2299-5. Epub 2021 Jan 11. Curr Med Sci. 2020. PMID: 33428146
-
Minimally Invasive Posterior Cervical Foraminotomy as an Alternative to Anterior Cervical Discectomy and Fusion for Unilateral Cervical Radiculopathy: A Systematic Review and Meta-analysis.Spine (Phila Pa 1976). 2019 Dec 15;44(24):1731-1739. doi: 10.1097/BRS.0000000000003156. Spine (Phila Pa 1976). 2019. PMID: 31343619
-
Posterior Cervical Foraminotomy Via Full-Endoscopic Versus Microendoscopic Approach for Radiculopathy: A Systematic Review and Meta-analysis.Pain Physician. 2019 Jan;22(1):41-52. Pain Physician. 2019. PMID: 30700067
Cited by
-
Successful outcomes following transforaminal epidural steroid injections for C4/5 cervical disc prolapse associated with profound neurological deficit.Eur Spine J. 2017 May;26(Suppl 1):207-212. doi: 10.1007/s00586-017-5031-9. Epub 2017 Mar 27. Eur Spine J. 2017. PMID: 28349269
-
[Research progress in minimally invasive treatment of cervical nerve root canal stenosis under total endoscope].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020 Feb 15;34(2):256-259. doi: 10.7507/1002-1892.201906026. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020. PMID: 32030960 Free PMC article. Chinese.
-
Comparison of Percutaneous Endoscopic Cervical Keyhole Foraminotomy versus Microscopic Anterior Cervical Discectomy and Fusion for Single Level Unilateral Cervical Radiculopathy.Int J Gen Med. 2022 Aug 29;15:6897-6907. doi: 10.2147/IJGM.S378837. eCollection 2022. Int J Gen Med. 2022. PMID: 36061960 Free PMC article.
-
Minimally invasive cervical laminoforaminotomy - Technique and outcomes.J Craniovertebr Junction Spine. 2021 Oct-Dec;12(4):361-367. doi: 10.4103/jcvjs.jcvjs_137_21. Epub 2021 Dec 11. J Craniovertebr Junction Spine. 2021. PMID: 35068817 Free PMC article.
-
Clinical and Radiological Outcomes of Day-care Posterior Foraminotomy and Decompression of the Cervical Spine.Asian J Neurosurg. 2018 Oct-Dec;13(4):1118-1122. doi: 10.4103/ajns.AJNS_14_17. Asian J Neurosurg. 2018. PMID: 30459879 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
