

Protracted primary cytomegalovirus infection presenting as ileoanal pouchitis in a non-immunosuppressed patient: a case report
- PMID: 24885004
- PMCID: PMC4061925
- DOI: 10.1186/1752-1947-8-163
Protracted primary cytomegalovirus infection presenting as ileoanal pouchitis in a non-immunosuppressed patient: a case report
Abstract
Introduction: Pouchitis often occurs after proctocolectomy and ileal pouch-anal anastomosis for ulcerative colitis. It is usually deemed idiopathic and commonly responds to antibacterial therapy. To date, only a few cases of cytomegalovirus pouchitis have been documented, and only a single report describes pouchitis in a case of assumed primary cytomegalovirus infection.
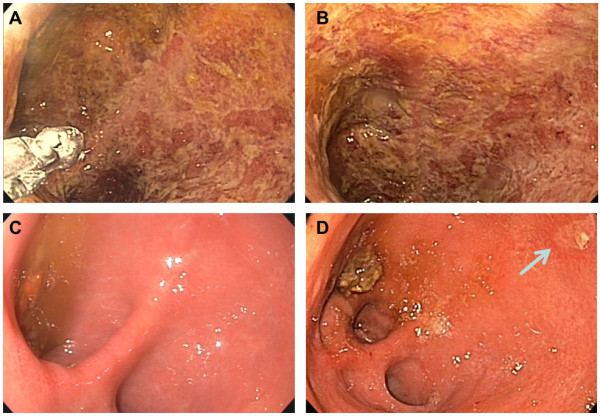
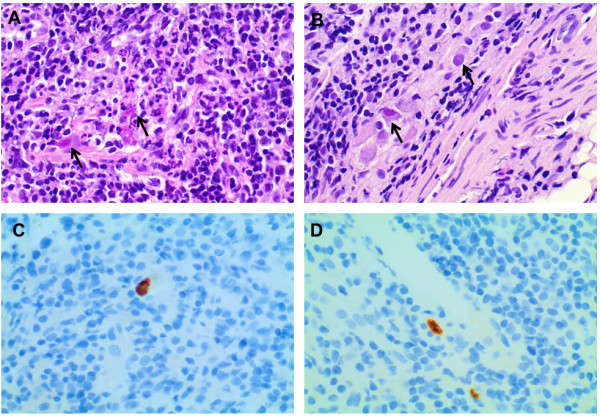
Case presentation: A 26-year-old Caucasian woman underwent proctocolectomy and ileal pouch-anal anastomosis for refractory ulcerative colitis and adenocarcinoma. After 28 months she developed bloody diarrhoea, abdominal pain, fever, nausea and general malaise suggesting severe pouchitis. Antibiotic treatment reduced humoral inflammation, but failed to resolve her fever. A pouchoscopy revealed distinct pouchitis, and cytomegalovirus infection was diagnosed from pouch biopsies by polymerase chain reaction as well as conventional histology and immunohistochemistry. The infection was confirmed in her blood by polymerase chain reaction and pp65 antigen test, and was clearly defined as the 'primary' infection by serial serological tests. Intravenous treatment with ganciclovir (10mg/kg body weight/day) led to resolution of symptoms and negative cytomegalovirus deoxyribonucleic acid and pp65 within a few days. When symptoms and laboratory evidence of cytomegalovirus infection recurred a few days after completing 20 days of therapy with ganciclovir and valganciclovir, a second course of ganciclovir treatment was initiated.
Conclusions: Cytomegalovirus infection of the ileoanal pouch is an important differential diagnosis of pouchitis even in non-immunosuppressed patients and can be treated with ganciclovir.
Figures
Similar articles
-
Misdiagnosis of specific cytomegalovirus infection of the ileoanal pouch as refractory idiopathic chronic pouchitis: report of two cases.Dis Colon Rectum. 1999 Jan;42(1):117-20. doi: 10.1007/BF02235196. Dis Colon Rectum. 1999. PMID: 10211531
-
Cytomegalovirus pouchitis in a patient with Crohn's disease.BMJ Case Rep. 2014 Jul 17;2014:bcr2014205374. doi: 10.1136/bcr-2014-205374. BMJ Case Rep. 2014. PMID: 25035450 Free PMC article.
-
Cytomegalovirus infection as a cause of ileoanal pouchitis.Dis Colon Rectum. 2000 Jan;43(1):113-4. doi: 10.1007/BF02237255. Dis Colon Rectum. 2000. PMID: 10813135 No abstract available.
-
Pouchitis after ileal pouch-anal anastomosis in ulcerative colitis: Diagnosis, management, risk factors, and incidence.Dig Endosc. 2017 Jan;29(1):26-34. doi: 10.1111/den.12744. Epub 2016 Nov 7. Dig Endosc. 2017. PMID: 27681447 Review.
-
[Differential indications for ileoanal pouch anastomosis : Ulcerative colitis, familial adenomatous polyposis, synchronous colorectal cancer - Crohn's disease, constipation].Chirurg. 2017 Jul;88(7):555-558. doi: 10.1007/s00104-017-0421-4. Chirurg. 2017. PMID: 28405717 Review. German.
Cited by
-
Prevalence of cytomegalovirus infection in patients with ulcerative colitis: a prospective cross-sectional study in Tehran, Iran.Iran J Microbiol. 2018 Oct;10(5):342-347. Iran J Microbiol. 2018. PMID: 30675331 Free PMC article.
References
-
- Tribonias G, Karmiris K, Giannikaki E, Konstantinidis K, Voudoukis E, Theodoropoulou A, Vardas E, Paspatis GA. Detection of CMV in pouch mucosa in a patient with acute pouchitis: the real enemy or an innocent bystander? J Crohns Colitis. 2012;6:728–729. doi: 10.1016/j.crohns.2012.02.011. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
