

Retraining and assessing hand movement after stroke using the MusicGlove: comparison with conventional hand therapy and isometric grip training
- PMID: 24885076
- PMCID: PMC4022276
- DOI: 10.1186/1743-0003-11-76
Retraining and assessing hand movement after stroke using the MusicGlove: comparison with conventional hand therapy and isometric grip training
Abstract
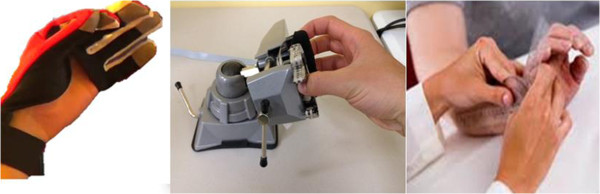
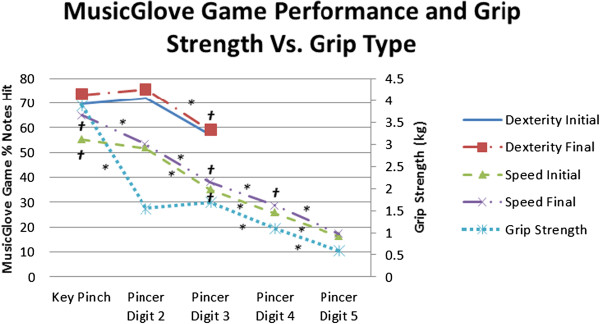
Background: It is thought that therapy should be functional, be highly repetitive, and promote afferent input to best stimulate hand motor recovery after stroke, yet patients struggle to access such therapy. We developed the MusicGlove, an instrumented glove that requires the user to practice gripping-like movements and thumb-finger opposition to play a highly engaging, music-based, video game. The purpose of this study was to 1) compare the effect of training with MusicGlove to conventional hand therapy 2) determine if MusicGlove training was more effective than a matched form of isometric hand movement training; and 3) determine if MusicGlove game scores predict clinical outcomes.
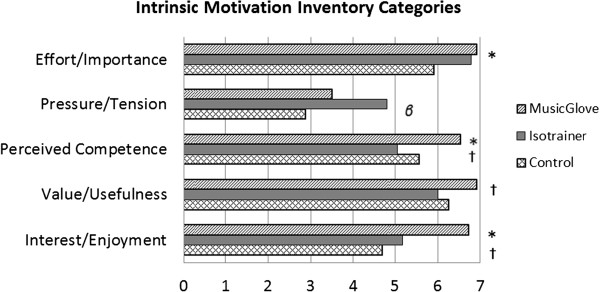
Methods: 12 chronic stroke survivors with moderate hemiparesis were randomly assigned to receive MusicGlove, isometric, and conventional hand therapy in a within-subjects design. Each subject participated in six one-hour treatment sessions three times per week for two weeks, for each training type, for a total of 18 treatment sessions. A blinded rater assessed hand impairment before and after each training type and at one-month follow-up including the Box and Blocks (B & B) test as the primary outcome measure. Subjects also completed the Intrinsic Motivation Inventory (IMI).
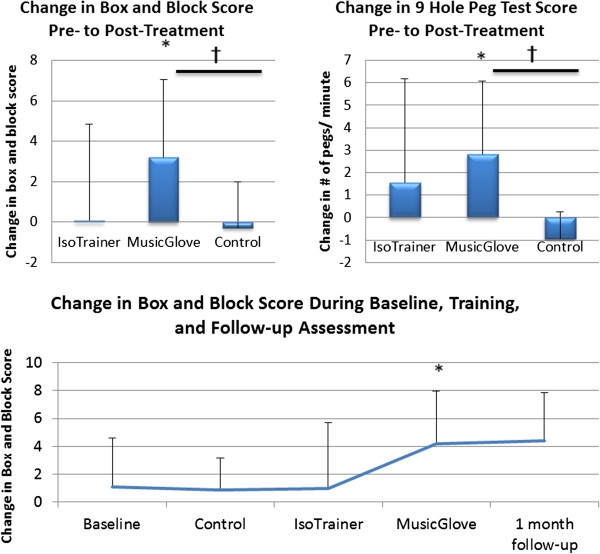
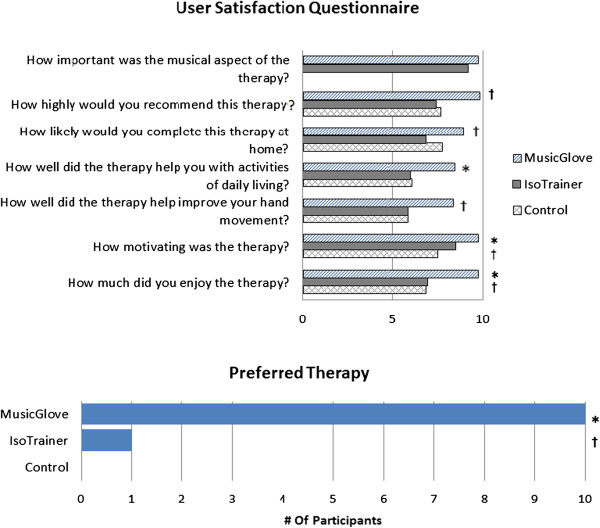
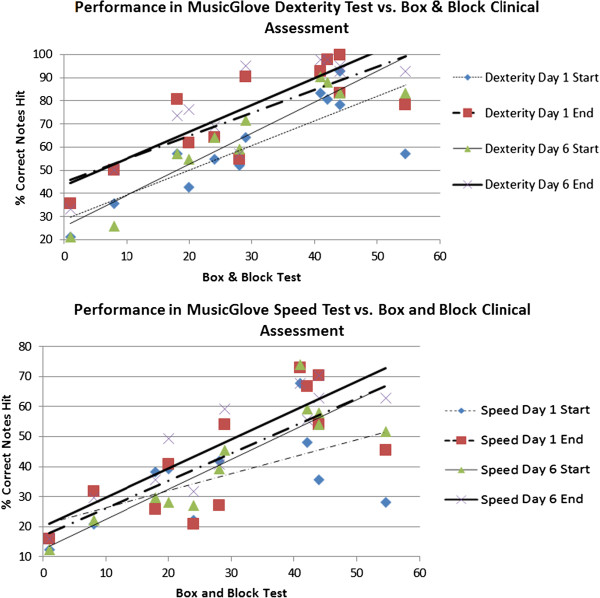
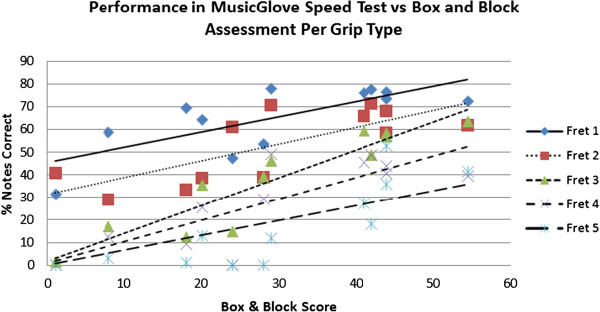
Results: Subjects improved hand function related to grasping small objects more after MusicGlove compared to conventional training, as measured by the B & B score (improvement of 3.21±3.82 vs. -0.29±2.27 blocks; P=0.010) and the 9 Hole Peg test (improvement of 2.14±2.98 vs. -0.85±1.29 pegs/minute; P=0.005). There was no significant difference between training types in the broader assessment batteries of hand function. Subjects benefited less from isometric therapy than MusicGlove training, but the difference was not significant (P>0.09). Subjects sustained improvements in hand function at a one month follow-up, and found the MusicGlove more motivating than the other two therapies, as measured by the IMI. MusicGlove games scores correlated strongly with the B & B score.
Conclusions: These results support the hypothesis that hand therapy that is engaging, incorporates high numbers of repetitions of gripping and thumb-finger opposition movements, and promotes afferent input is a promising approach to improving an individual's ability to manipulate small objects. The MusicGlove provides a simple way to access such therapy.
Figures

References
-
- Dobkin BH. Neurologic Rehabilitation. Philadelphia: FA Davis Company; 1996.
-
- Bard G, Hirschberg GG. “Recovery of voluntary motion in upper extremity following hemiplegia”. Arch Phys Med Rehabil. 1965;46:567–572. - PubMed
-
- Parker VM, Wade DT, Langton Hewer R. “Loss of arm function after stroke: measurement, frequency, and recovery”. Int Rehabil Med. 1986;8(2):69–73. - PubMed
-
- Sawaki L. “Use-dependent plasticity of the human motor cortex in health and disease”. IEEE Eng Med Biol Mag. 2005;24(1):36–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
