

Perinatal mortality by gestational week and size at birth in singleton pregnancies at and beyond term: a nationwide population-based cohort study
- PMID: 24885576
- PMCID: PMC4037279
- DOI: 10.1186/1471-2393-14-172
Perinatal mortality by gestational week and size at birth in singleton pregnancies at and beyond term: a nationwide population-based cohort study
Abstract
Background: Whether gestational age per se increases perinatal mortality in post-term pregnancy is unclear. We aimed at assessing gestational week specific perinatal mortality in small-for-gestational-age (SGA) and non-SGA term and post-term gestations, and specifically to evaluate whether the relation between post-term gestation and perinatal mortality differed before and after ultrasound was introduced as the standard method of gestational age estimation.
Methods: A population-based cohort study, using data from the Medical Birth Registry of Norway (MBRN), 1967-2006, was designed. Singleton births at 37 through 44 gestational weeks (n = 1 855 682), excluding preeclampsia, diabetes and fetal anomalies, were included. Odds ratios (OR) with 95% confidence intervals (CI) for perinatal mortality and stillbirth in SGA and non-SGA births by gestational week were calculated.
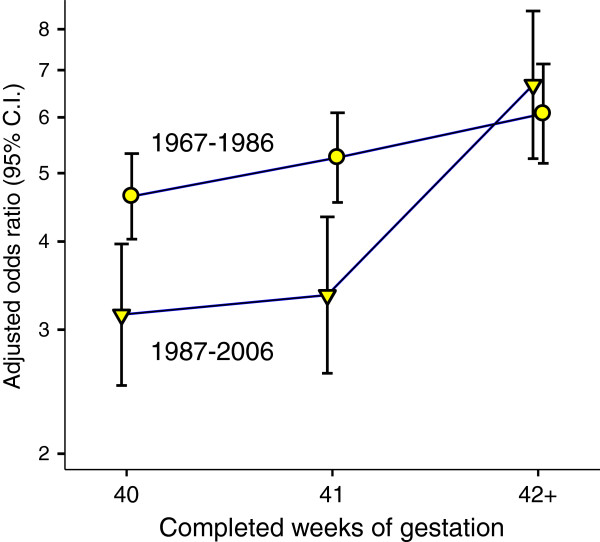
Results: SGA infants judged post-term by LMP had significantly higher perinatal mortality than post-term non-SGA infants at 40 weeks, independent of time period (highest during 1999-2006 [OR 9.8, 95% CI: 5.7-17.0]). When comparing years before (1967-1986) versus after (1987-2006) ultrasound was introduced, there was no decrease in the excess mortality for post-term SGA versus non-SGA births (ORs from 6.1 [95% CI: 5.2-7.1] to 6.7 [5.2-8.5]), while mortality at 40 weeks decreased significantly (ORs from 4.6, [4.0-5.3] to 3.2 [2.5-3.9]). When assessing stillbirth risk (1999-2006), more than 40% of SGA stillbirths (11/26) judged to be ≥41 weeks by LMP were shifted to lower gestational ages using ultrasound estimation.
Conclusions: Mortality risk in post-term infants was strongly associated with growth restriction. Such infants may erroneously be judged younger than they are when using ultrasound estimation, so that the routine assessment for fetal wellbeing in the prolonged gestation may be given too late.
Figures
References
-
- World Health Organisation. The Prevention of Perinatal Mortality and Morbidity. Geneva, Switzerland: WHO Technical Report Series; Report 457; 1970. - PubMed
-
- FIGO. Report of the FIGO Subcommittee on Perinatal Epidemiology and Health Statistics. London: FIGO; 1986.
-
- Heimstad R. Post-term Pregnancy. Trondheim: Norwegian University of Science and Technology; 2007.
-
- Caughey AB, Stotland NE, Washington AE, Escobar GJ. Who is at risk for prolonged and postterm pregnancy? Am J Obstet Gynecol. 2009;200(6):683–e681-685. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
