

Quantification of tumour budding, lymphatic vessel density and invasion through image analysis in colorectal cancer
- PMID: 24885583
- PMCID: PMC4098951
- DOI: 10.1186/1479-5876-12-156
Quantification of tumour budding, lymphatic vessel density and invasion through image analysis in colorectal cancer
Abstract
Background: Tumour budding (TB), lymphatic vessel density (LVD) and lymphatic vessel invasion (LVI) have shown promise as prognostic factors in colorectal cancer (CRC) but reproducibility using conventional histopathology is challenging. We demonstrate image analysis methodology to quantify the histopathological features which could permit standardisation across institutes and aid risk stratification of Dukes B patients.
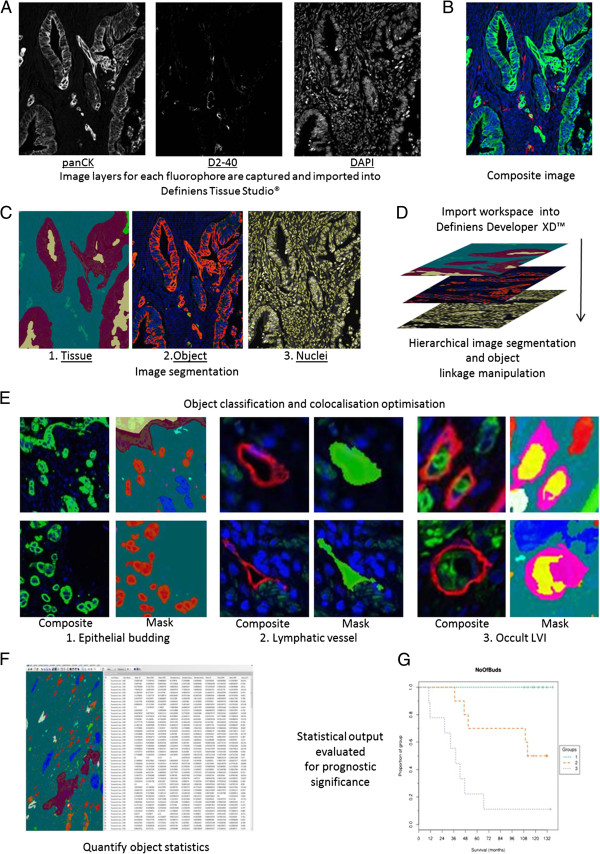
Methods: Multiplexed immunofluorescence of pan-cytokeratin, D2-40 and DAPI identified epithelium, lymphatic vessels and all nuclei respectively in tissue sections from 50 patients diagnosed with Dukes A (n = 13), Dukes B (n = 29) and Dukes C (n = 8) CRC. An image analysis algorithm was developed and performed, on digitised images of the CRC tissue sections, to quantify TB, LVD, and LVI at the invasive front.
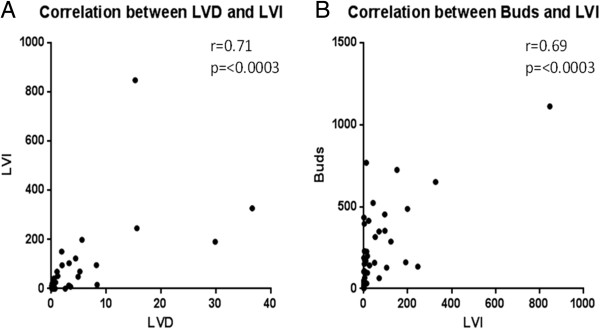
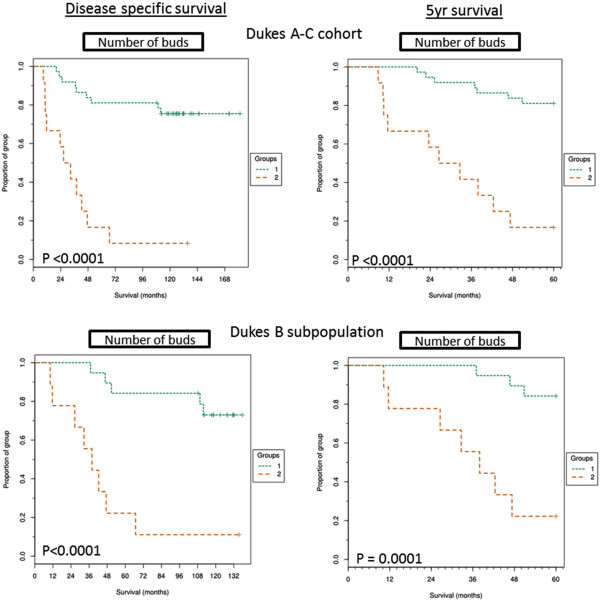
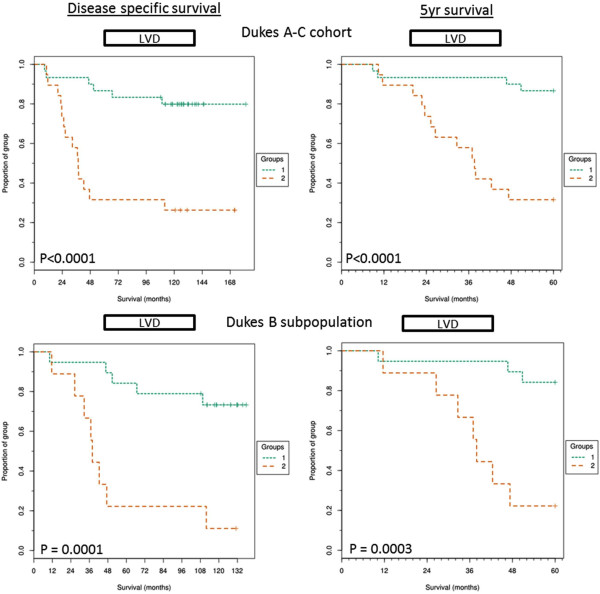
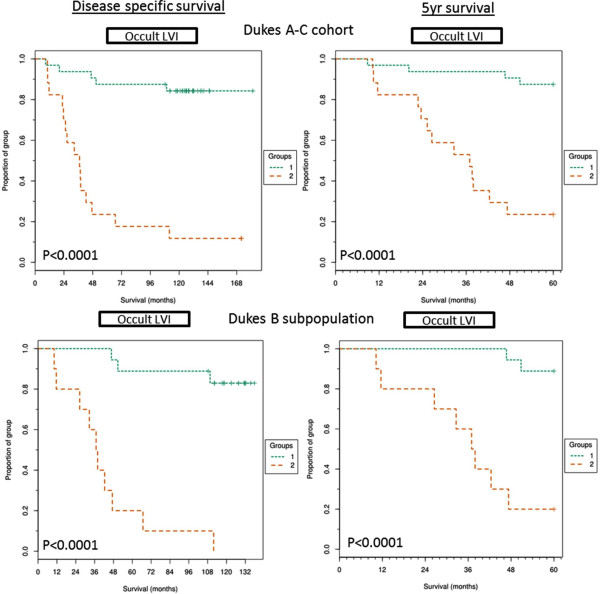
Results: TB (HR =5.7; 95% CI, 2.38-13.8), LVD (HR =5.1; 95% CI, 2.04-12.99) and LVI (HR =9.9; 95% CI, 3.57-27.98) were successfully quantified through image analysis and all were shown to be significantly associated with poor survival, in univariate analyses. LVI (HR =6.08; 95% CI, 1.17-31.41) is an independent prognostic factor within the study and was correlated to both TB (Pearson r =0.71, p <0.0003) and LVD (Pearson r =0.69, p <0.0003).
Conclusion: We demonstrate methodology through image analysis which can standardise the quantification of TB, LVD and LVI from a single tissue section while decreasing observer variability. We suggest this technology is capable of stratifying a high risk Dukes B CRC subpopulation and we show the three histopathological features to be of prognostic significance.
Figures
References
-
- Standards and Datasets for Reporting Cancers Dataset for colorectal cancer. 2. 2007. [ http://www.rcpath.org/Resources/RCPath/Migrated%20Resources/Documents/G/...]
-
- Lan YT, Yang SH, Chang SC, Liang WY, Li AF, Wang HS, Jiang JK, Chen WS, Lin TC, Lin JK. Analysis of the seventh edition of American Joint Committee on colon cancer staging. Int J Colorectal Dis. 2012;27:657–663. - PubMed
-
- Poston GJ, Tait D, O'Connell S, Bennett A, Berendse S. Diagnosis and management of colorectal cancer: summary of NICE guidance. BMJ. 2011;343:d6751. - PubMed
-
- O'Connell JB, Maggard MA, Ko CY. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J Natl Cancer Inst. 2004;96:1420–1425. - PubMed
-
- Huh JW, Lee JH, Kim HR, Kim YJ. Prognostic significance of lymphovascular or perineural invasion in patients with locally advanced colorectal cancer. Am J Surg. 2013;206:758–763. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
