

Leukemoid reaction and autocrine growth of bladder cancer induced by paraneoplastic production of granulocyte colony-stimulating factor--a potential neoplastic marker: a case report and review of the literature
- PMID: 24885603
- PMCID: PMC4055228
- DOI: 10.1186/1752-1947-8-147
Leukemoid reaction and autocrine growth of bladder cancer induced by paraneoplastic production of granulocyte colony-stimulating factor--a potential neoplastic marker: a case report and review of the literature
Abstract
Introduction: Granulocyte colony-stimulating factor produced by nonhematopoietic malignant cells is able to induce a leukemoid reaction by excessive stimulation of leukocyte production. Expression of granulocyte colony-stimulating factor and its functional receptors have been confirmed in bladder cancer cells. In vitro studies have demonstrated that granulocyte colony-stimulating factor/receptor exhibits a high affinity binding and this biological axis increases proliferation of the carcinoma. Urothelial carcinoma of the bladder is rarely associated with a leukemoid reaction and autocrine growth induced by paraneoplastic production of granulocyte colony-stimulating factor. In the world literature, there have been less than 35 cases reported in the last 35 years. The clinicopathological aspects, biology, prognosis and management of granulocyte colony-stimulating factor-secreting bladder cancers are poorly understood.
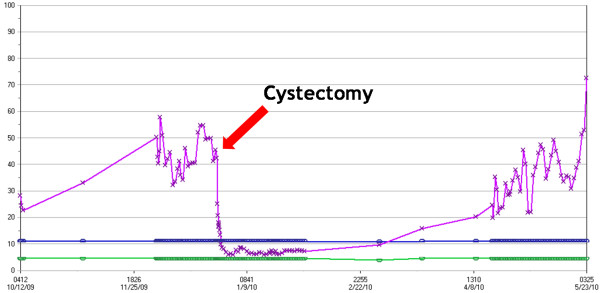
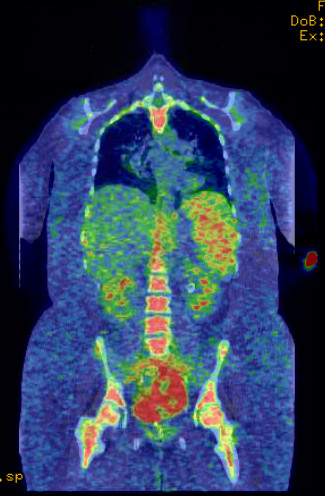
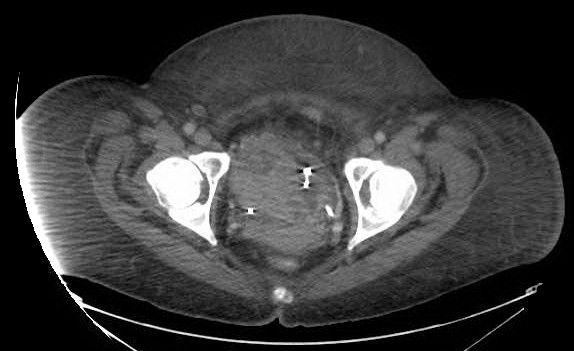
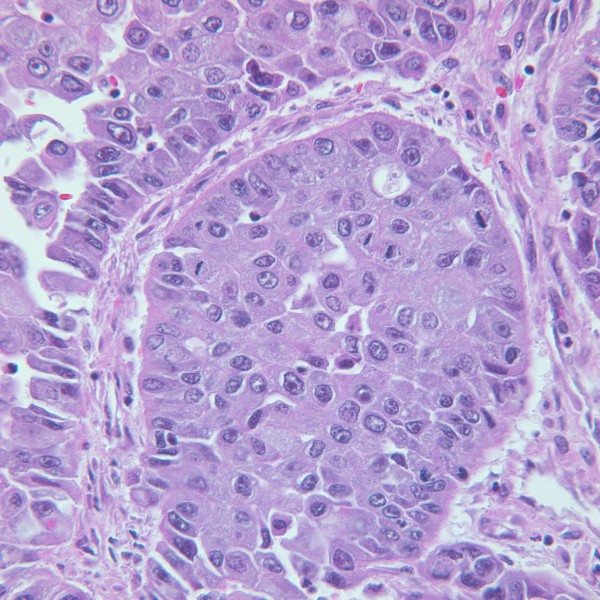
Case presentation: A 39-year-old Caucasian woman with an invasive high-grade urothelial carcinoma presented with hematuria and low-grade fevers. Laboratory tests revealed an elevated white blood cell count and absolute neutrophil count and an elevated 24-hour urine protein. Upon further evaluation she was found to have locally advanced high-grade urothelial carcinoma without nodal or distant metastasis. Her serum granulocyte colony-stimulating factor level was 10 times the normal limit. This led to the diagnosis of a paraneoplastic leukemoid reaction. Her white blood cell count immediately normalized after cystectomy but increased in concordance with recurrence of her disease. Unfortunately, she rapidly progressed and expired within 10 months from the time of first diagnosis.
Conclusions: This is one of the few cases reported that illustrates the existence of a distinct and highly aggressive subtype of bladder cancer which secretes granulocyte colony-stimulating factor. Patients presenting with a leukemoid reaction should be tested for granulocyte colony-stimulating factor/receptor biological axis. Moreover, granulocyte colony-stimulating factor could be a potential neoplastic marker as it can follow the clinical course of the underlying tumor and thus be useful for monitoring its evolution. Neoadjuvant chemotherapy should be considered in these patients due to the aggressive nature of these tumors. With a better understanding of the biology, this autocrine growth signal could be a potential target for therapy in future.
Figures
References
-
- Tachibana M, Miyakawa A, Tazaki H, Nakamura K, Kubo A, Hata J, Nishi T, Amano Y. Autocrine growth of transitional cell carcinoma of the bladder induced by granulocyte-colony stimulating factor. Cancer Res. 1995;55:3438–3443. - PubMed
-
- Demetri GD, Griffin JD. Granulocyte colony-stimulating factor and its receptor. Blood. 1991;78:2791–2808. - PubMed
-
- Sato K, Terada K, Sugiyama T, Masuda H, Kakinuma H, Kato T. Granulocyte colony-stimulating factor produced by bladder carcinoma of a patient with leukemoid reaction did not affect proliferation of the tumor cells. J Urol. 1994;151:1687–1690. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
