

Outcome of artemether-lumefantrine treatment for uncomplicated malaria in HIV-infected adult patients on anti-retroviral therapy
- PMID: 24885714
- PMCID: PMC4051371
- DOI: 10.1186/1475-2875-13-205
Outcome of artemether-lumefantrine treatment for uncomplicated malaria in HIV-infected adult patients on anti-retroviral therapy
Abstract
Background: Malaria and HIV infections are both highly prevalent in sub-Saharan Africa, with HIV-infected patients being at higher risks of acquiring malaria. The majority of antiretroviral (ART) and anti-malarial drugs are metabolized by the CYP450 system, creating a chance of drug-drug interaction upon co-administration. Limited data are available on the effectiveness of the artemether-lumefantrine combination (AL) when co-administered with non-nucleoside reverse transcriptase inhibitors (NNRTIs). The aim of this study was to compare anti-malarial treatment responses between HIV-1 infected patients on either nevirapine- or efavirenz-based treatment and those not yet on ART (control-arm) with uncomplicated falciparum malaria, treated with AL.
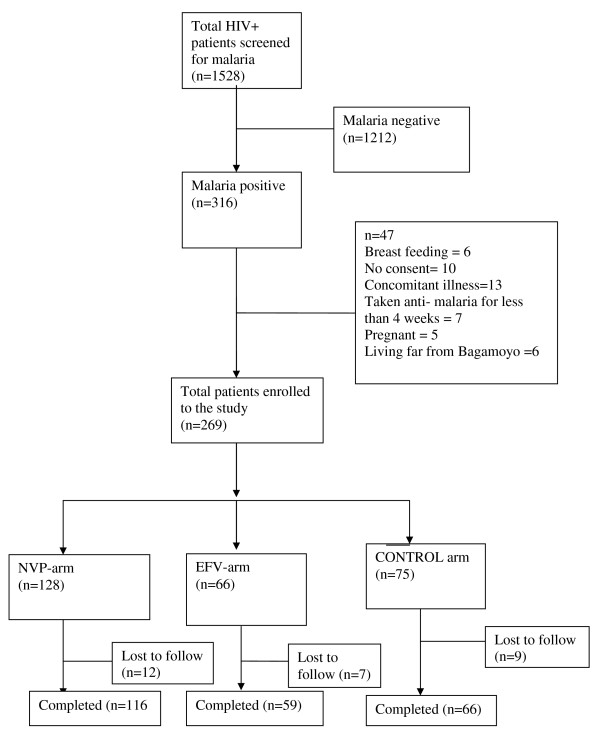
Method: This was a prospective, non-randomized, open-label study conducted in Bagamoyo district, with three arms of HIV-infected adults: efavirenz-based treatment arm (EFV-arm) n = 66, nevirapine-based treatment arm (NVP-arm) n = 128, and control-arm n = 75, with uncomplicated malaria. All patients were treated with AL and followed up for 28 days. The primary outcome measure was an adequate clinical and parasitological response (ACPR) after treatment with AL by day 28.
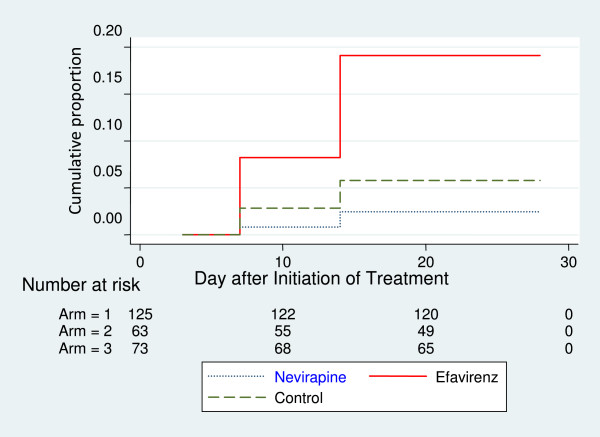
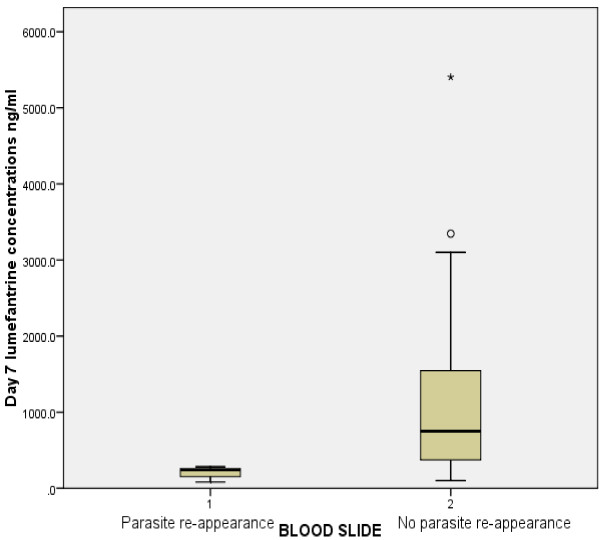
Results: Day 28 ACPR was 97.6%, 82.5% and 94.5% for the NVP-arm, EFV-arm and control-arm, respectively. No early treatment or late parasitological failure was reported. The cumulative risk of recurrent parasitaemia was >19-fold higher in the EFV-arm than in the control-arm (Hazard ratio [HR], 19.11 [95% confidence interval {CI}, 10.5-34.5]; P < 0.01). The cumulative risk of recurrent parasitaemia in the NVP-arm was not significantly higher than in the control-arm ([HR], 2.44 [95% {CI}, 0.79-7.6]; P = 0.53). The median (IQR) day 7 plasma concentrations of lumefantrine for the three arms were: 1,125 ng/m (638.8-1913), 300.4 ng/ml (220.8-343.1) and 970 ng/ml (562.1-1729) for the NVP-arm, the EFV-arm and the control-arm, respectively (P < 0.001). In all three arms, the reported adverse events were mostly mild.
Conclusion: After 28 days of follow-up, AL was statistically safe and effective in the treatment of uncomplicated malaria in the NVP-arm. The results of this study also provide an indication of the possible impact of EFV on the performance of AL and the likelihood of it affecting uncomplicated falciparum malaria treatment outcome.
Figures
Similar articles
-
The influence of nevirapine and efavirenz-based anti-retroviral therapy on the pharmacokinetics of lumefantrine and anti-malarial dose recommendation in HIV-malaria co-treatment.Malar J. 2015 Apr 25;14:179. doi: 10.1186/s12936-015-0695-2. Malar J. 2015. PMID: 25906774 Free PMC article.
-
Interaction between artemether-lumefantrine and nevirapine-based antiretroviral therapy in HIV-1-infected patients.Antimicrob Agents Chemother. 2011 Dec;55(12):5616-23. doi: 10.1128/AAC.05265-11. Epub 2011 Sep 26. Antimicrob Agents Chemother. 2011. PMID: 21947399 Free PMC article. Clinical Trial.
-
CYP2B6*6 genotype and high efavirenz plasma concentration but not nevirapine are associated with low lumefantrine plasma exposure and poor treatment response in HIV-malaria-coinfected patients.Pharmacogenomics J. 2016 Feb;16(1):88-95. doi: 10.1038/tpj.2015.37. Epub 2015 May 12. Pharmacogenomics J. 2016. PMID: 25963334
-
Efficacy of artemisinin-based combination therapy (ACT) in people living with HIV (PLHIV) diagnosed with uncomplicated Plasmodium falciparum malaria in Africa: a WWARN systematic review.Malar J. 2025 May 16;24(1):153. doi: 10.1186/s12936-025-05393-8. Malar J. 2025. PMID: 40380136 Free PMC article.
-
Artemether-lumefantrine: an option for malaria.Ann Pharmacother. 2012 Apr;46(4):567-77. doi: 10.1345/aph.1Q539. Epub 2012 Apr 10. Ann Pharmacother. 2012. PMID: 22496476 Review.
Cited by
-
The epidemiological impact of HIV antiretroviral therapy on malaria in children.AIDS. 2015 Feb 20;29(4):473-82. doi: 10.1097/QAD.0000000000000550. AIDS. 2015. PMID: 25486414 Free PMC article.
-
"Every drug goes to treat its own disease…" - a qualitative study of perceptions and experiences of taking anti-retrovirals concomitantly with anti-malarials among those affected by HIV and malaria in Tanzania.Malar J. 2014 Dec 13;13:491. doi: 10.1186/1475-2875-13-491. Malar J. 2014. PMID: 25495956 Free PMC article.
-
Efficacy and safety of artemether-lumefantrine as treatment for Plasmodium falciparum uncomplicated malaria in adult patients on efavirenz-based antiretroviral therapy in Zambia: an open label non-randomized interventional trial.Malar J. 2019 May 24;18(1):180. doi: 10.1186/s12936-019-2818-7. Malar J. 2019. PMID: 31126288 Free PMC article. Clinical Trial.
-
Antiretroviral Choice for HIV Impacts Antimalarial Exposure and Treatment Outcomes in Ugandan Children.Clin Infect Dis. 2016 Aug 1;63(3):414-22. doi: 10.1093/cid/ciw291. Epub 2016 May 3. Clin Infect Dis. 2016. PMID: 27143666 Free PMC article.
-
Efavirenz-Based Antiretroviral Therapy Reduces Artemether-Lumefantrine Exposure for Malaria Treatment in HIV-Infected Pregnant Women.J Acquir Immune Defic Syndr. 2020 Feb 1;83(2):140-147. doi: 10.1097/QAI.0000000000002237. J Acquir Immune Defic Syndr. 2020. PMID: 31929402 Free PMC article.
References
-
- World Health Organization. Malaria and HIV Interactions and Their Implications for Public Health Policy. [ http://whqlibdoc.who.int/publications/2005/9241593350.pdf]
-
- UNAIDS. Joint United Nations Programme on HIV/AIDS Global Report. UNAIDS report on the global AIDS epidemic 2012; [ http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo...]
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
